Clinical Report: Comparative Analysis of Adverse Pregnancy Outcomes Across Hypertensive Disorder Subtypes
Overview
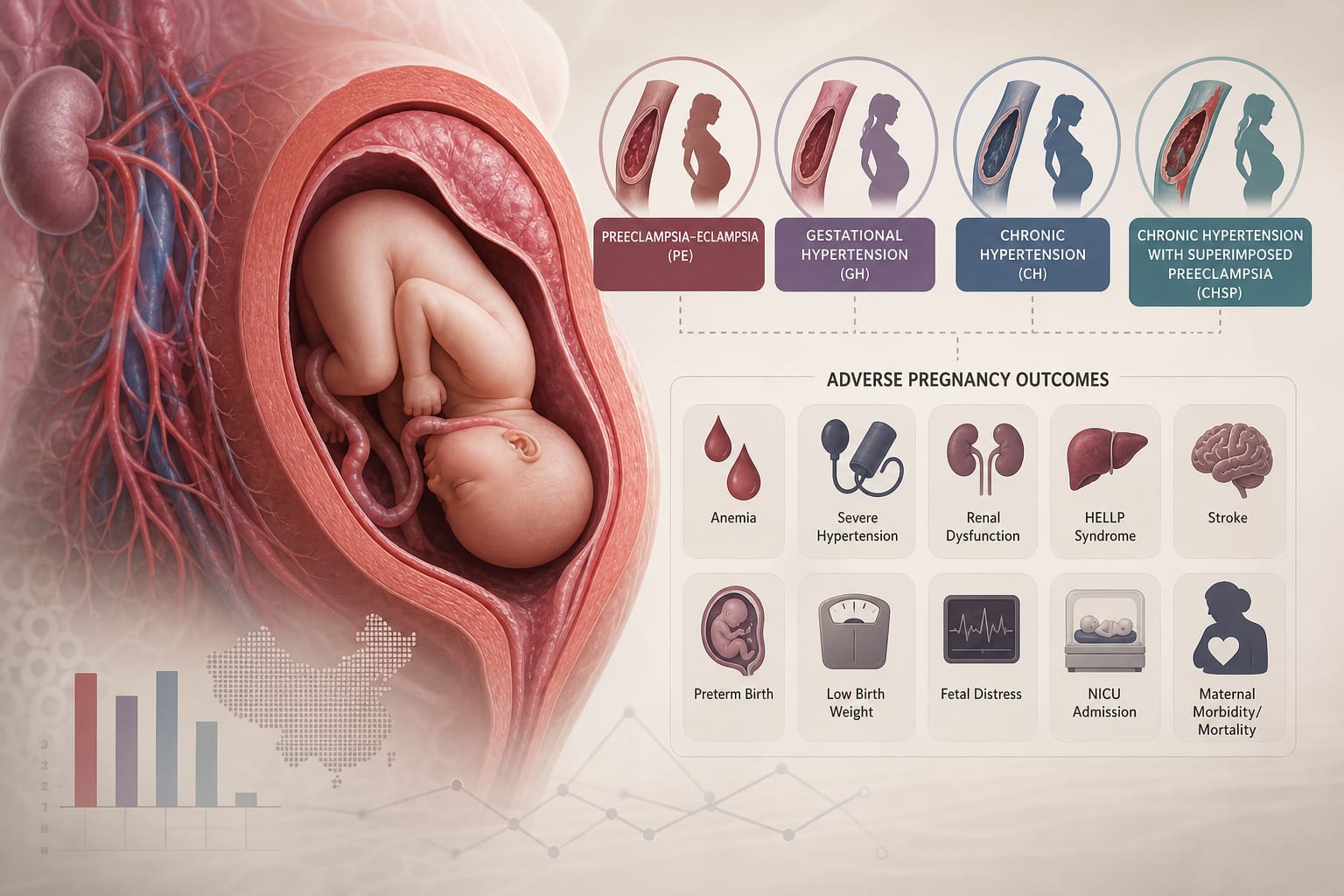
This study compares adverse pregnancy outcomes (APOs) among different subtypes of hypertensive disorders of pregnancy (HDP) using data from Hunan Province, China. Significant differences in the prevalence of various APOs were found, particularly highlighting the higher rates of complications in preeclampsia-eclampsia and chronic hypertension with superimposed preeclampsia.
Background
Hypertensive disorders of pregnancy (HDP) are prevalent complications affecting maternal and fetal health, with significant implications for pregnancy outcomes. The classification of HDP into subtypes such as preeclampsia-eclampsia and chronic hypertension is crucial for understanding the associated risks. Identifying differences in adverse pregnancy outcomes across these subtypes can inform clinical management and counseling.
Data Highlights
Outcome
Overall Prevalence
PE
CH
CHSP
GH
Anemia
30.78%
32.97%
-
-
-
Diabetes Mellitus
20.33%
-
25.27%
25.11%
-
Preterm Birth
19.53%
27.76%
-
37.01%
-
Low Birthweight
18.74%
27.72%
-
31.39%
-
Hemorrhage Disorder
9.07%
9.86%
-
-
-
Infection
4.71%
5.20%
-
5.05%
-
Stillbirth and Neonatal Death
2.38%
3.18%
-
6.64%
-
Maternal Near-Miss
1.57%
2.47%
-
2.31%
-
Key Findings
The study included 780,359 pregnant women, identifying 38,397 cases of HDP.
Preeclampsia-eclampsia (PE) accounted for 46.31% of HDP cases, while chronic hypertension with superimposed preeclampsia (CHSP) was the least common at 3.61%.
Significant differences in the prevalence of adverse pregnancy outcomes were observed across HDP subtypes, particularly for anemia, diabetes mellitus, and preterm birth.
CHSP and PE had higher rates of preterm birth and low birthweight compared to other subtypes.
Diabetes mellitus was more prevalent in chronic hypertension (CH) and CHSP than in PE.
Infection rates were notably higher in PE and CHSP compared to other subtypes.
Clinical Implications
Understanding the differences in adverse pregnancy outcomes among HDP subtypes can aid healthcare professionals in risk assessment and management strategies for pregnant women. This information is essential for clinical counseling and may guide future research directions.
Conclusion
The findings highlight the varying risks associated with different subtypes of hypertensive disorders of pregnancy, emphasizing the need for tailored clinical approaches. Further studies are warranted to explore these relationships in greater depth.