Clinical Report: Intracranial Involvement in Adult Rosai-Dorfman Disease
Overview
This comprehensive review and meta-analysis of 327 adult cases of intracranial Rosai-Dorfman Disease (RDD) highlights its rarity, diagnostic challenges, and treatment heterogeneity. Intracranial RDD typically presents as dural-based masses mimicking meningiomas, with diagnosis relying on histopathology. Surgical resection remains the primary treatment, though recurrence and the role of adjuvant therapies require further clarification.
Background
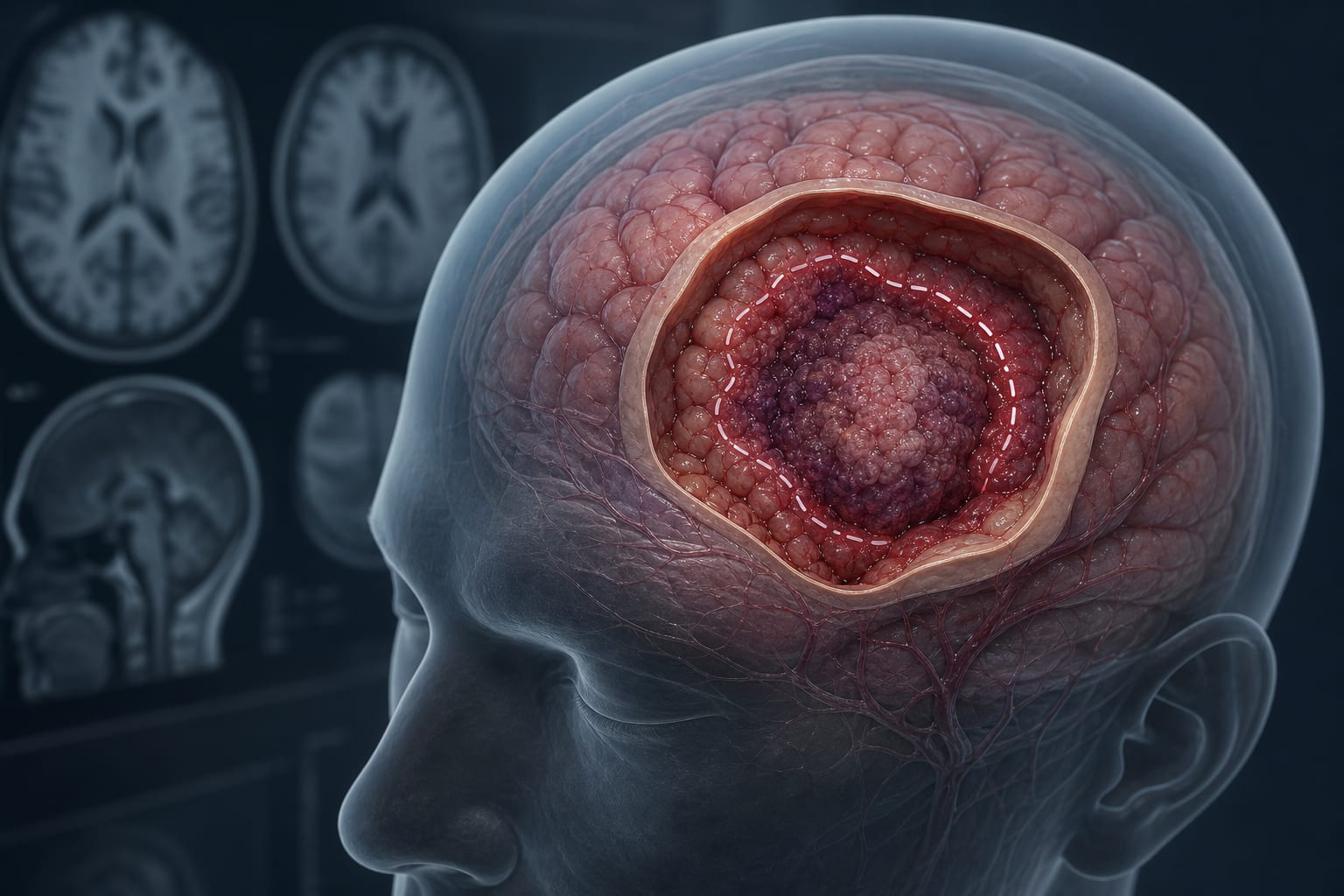
Rosai-Dorfman Disease is a rare non-Langerhans cell histiocytosis characterized by histiocyte accumulation, with an estimated prevalence of 1:200,000. Extranodal involvement occurs in over 40% of cases, and about 5% involve the central nervous system, predominantly intracranially. Intracranial RDD lesions often appear as dural-based enhancing masses indistinguishable from meningiomas on imaging, necessitating histopathologic confirmation. Clinical manifestations depend on lesion location and mass effect, including headaches, cranial neuropathies, seizures, and focal deficits.
Data Highlights
Parameter
Value
Number of cases analyzed
327
Estimated US incidence
~100 new cases/year
Prevalence
1:200,000
Percentage with CNS involvement
~5%
Percentage of CNS cases intracranial
~75%
Common immunohistochemical markers
S100+, CD68+, CD1a-
Key Findings
Intracranial RDD predominantly presents as dural-based, avidly enhancing masses radiographically similar to meningiomas.
Histopathology is essential for diagnosis, characterized by emperipolesis and immunopositivity for S100 and CD68, with absence of CD1a expression.
Surgical resection is the most common treatment, often improving symptoms, but recurrence or progression can occur.
Adjuvant therapies including corticosteroids, radiotherapy, and systemic agents are used variably, especially in multifocal or residual disease.
Adult intracranial RDD differs from pediatric and spinal disease, necessitating adult-specific data synthesis for clinical guidance.
Heterogeneity in treatment approaches and follow-up complicates outcome interpretation, highlighting the need for standardized reporting and collaborative research.
Clinical Implications
Clinicians should maintain a high index of suspicion for intracranial RDD in dural-based masses mimicking meningiomas, especially when histopathology reveals characteristic features. Surgical resection remains the cornerstone of management for accessible lesions, but careful long-term monitoring is essential due to potential recurrence. Multimodal treatment strategies may be considered for multifocal or unresectable disease, though evidence guiding adjuvant therapy remains limited.
Conclusion
Intracranial RDD in adults is a rare and diagnostically challenging entity requiring histopathologic confirmation. Surgical resection offers symptomatic relief, but variable outcomes and treatment heterogeneity underscore the need for prospective studies and standardized management protocols.
References
Rosai-Dorfman Disease Epidemiology and CNS Involvement -- Source Article
PRISMA Guidelines for Systematic Reviews -- Source Article
by Daniela A. Perez-Chadid, Aafreen Azmi, Jeremiah H. Wijaya, Temitope Oshinowo, Juan P. Avila-Madrigal, Aditi S. Gorthy, Sri Sai Lakshman Akkineni, Andrew Egladyous, Nemanja Novakovic, Morana Vojnic, Jonathan H. Sherman, Anil Nanda