Thrombotic Microangiopathy Associated with Carfilzomib Treatment: Singapore Case Series
Overview
This case series reports a 16.7% incidence of thrombotic microangiopathy (TMA) among 24 multiple myeloma patients treated with carfilzomib in Singapore. Four patients developed TMA with acute kidney injury and thrombocytopenia, with recovery following cessation of carfilzomib and supportive care.
Background
Carfilzomib is an irreversible proteasome inhibitor approved for relapsed multiple myeloma after prior therapies. Although phase II trials showed a favorable safety profile without specific signals of TMA, serious adverse events including anemia, thrombocytopenia, and renal impairment have been reported. TMA is a rare but serious complication characterized by microangiopathic hemolytic anemia, thrombocytopenia, and organ injury, often involving the kidneys. This report describes four cases of carfilzomib-associated TMA from two tertiary hospitals in Singapore.
Data Highlights
Patient
Age/Sex/Ethnicity
MM Status
Carfilzomib Dose
Time to TMA
Key Features
Treatment
Outcome
1
70/M/Chinese
Newly diagnosed
20 mg/m2 then 56 mg/m2
Cycle 2 Day 6
Fever, diarrhea, Hb drop 7.5 to 5.3 g/dl, platelets 105 to 5 ×10^9/l, creatinine 97 to 209 μmol/l, schistocytes, positive hemolysis
Carfilzomib stopped
Platelets and renal function recovered in 4 days
2
66/F/Chinese
Newly diagnosed
20 mg/m2 then 56 mg/m2
Cycle 2 Day 8
Hb drop 9 to 6.1 g/dl, platelets 351 to 55 ×10^9/l, creatinine 93 to 573 μmol/l, schistocytes, no infection
Carfilzomib stopped, temporary hemodialysis
Platelets recovered in 7 days, renal function normalized in 1 month
3
63/M/Chinese
Relapsed MM
27 mg/m2
Cycle 2 Day 15
Fever, diarrhea, parainfluenza B positive, platelets 224 to 3 ×10^9/l, creatinine 76 to 403 μmol/l, schistocytes
Carfilzomib held, monitored
Platelets recovered in 25 days, renal function in 60 days
4
58/M/Chinese
Relapsed MM
27 mg/m2
Cycle 3 Day 7
Fever, decreased urine output, Hb 9.1 to 5.9 g/dl, platelets 92 to 15 ×10^9/l, creatinine 277 to 1133 μmol/l, schistocytes
Carfilzomib stopped, hemodialysis
Platelets recovered in 10 days, renal function pending
Key Findings
Four cases of TMA occurred among 24 patients treated with carfilzomib, indicating a 16.7% incidence in this cohort.
TMA presented with acute kidney injury, thrombocytopenia, hemolytic anemia, and schistocytes on blood film.
Two patients had newly diagnosed multiple myeloma receiving frontline carfilzomib at 56 mg/m2; two had relapsed disease receiving 27 mg/m2.
Concurrent viral upper respiratory tract infections were noted in two patients at TMA onset.
All patients recovered platelet counts; three recovered renal function after cessation of carfilzomib and supportive care; one patient’s renal function remained impaired at report time.
No hypertension or proteinuria was observed, suggesting a mechanism distinct from VEGF inhibition-related TMA.
Clinical Implications
Clinicians should be vigilant for signs of TMA in patients receiving carfilzomib, especially with sudden anemia, thrombocytopenia, and renal impairment. Early recognition and prompt discontinuation of carfilzomib can lead to recovery of hematologic and renal parameters. Supportive care including temporary hemodialysis may be necessary, and rechallenge with carfilzomib is not recommended after TMA occurrence.
Conclusion
Carfilzomib-associated TMA, although rare, can occur early during treatment and may present with severe hematologic and renal abnormalities. Awareness and timely management are critical to improve outcomes in affected multiple myeloma patients.
References
Dimopoulos et al. 2012 -- Carfilzomib in relapsed multiple myeloma
Stewart et al. 2015 -- Safety profile of carfilzomib in MM
Chng et al. 2020 -- Carfilzomib-associated TMA case reports
by Y Chen, M Ooi, S F Lim, A Lin, J Lee, C Nagarajan, C Phipps, Y S Lee, N F Grigoropoulos, Z Lao, S Surendran, E M Teh, Y T Goh, W J Chng, S K Gopalakrishnan
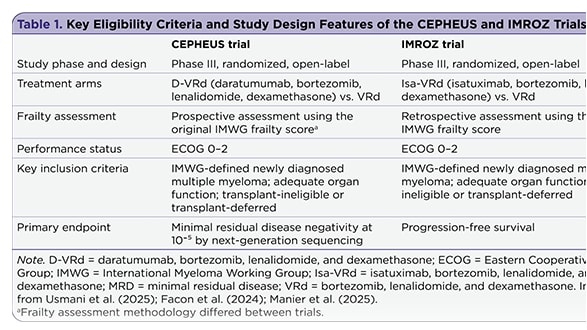
The management of newly diagnosed transplant-ineligible multiple myeloma remains challenging, in part due to the complexity of treatment decisions for frail patients. Recent subgroup analyses provide insight into whether quadruplet therapy may offer advantages over triplet therapy in this population.