Development and internal validation of a nomogram for early prediction of hospital-acquired ESKAPE colonization or infection in very preterm infants using indicators available within 24 hours - Report - MDSpire
Advertisement
Development and internal validation of a nomogram for early prediction of hospital-acquired ESKAPE colonization or infection in very preterm infants using indicators available within 24 hours
Clinical Report: Nomogram for Early Detection of ESKAPE Infections in Preterm Infants
Overview
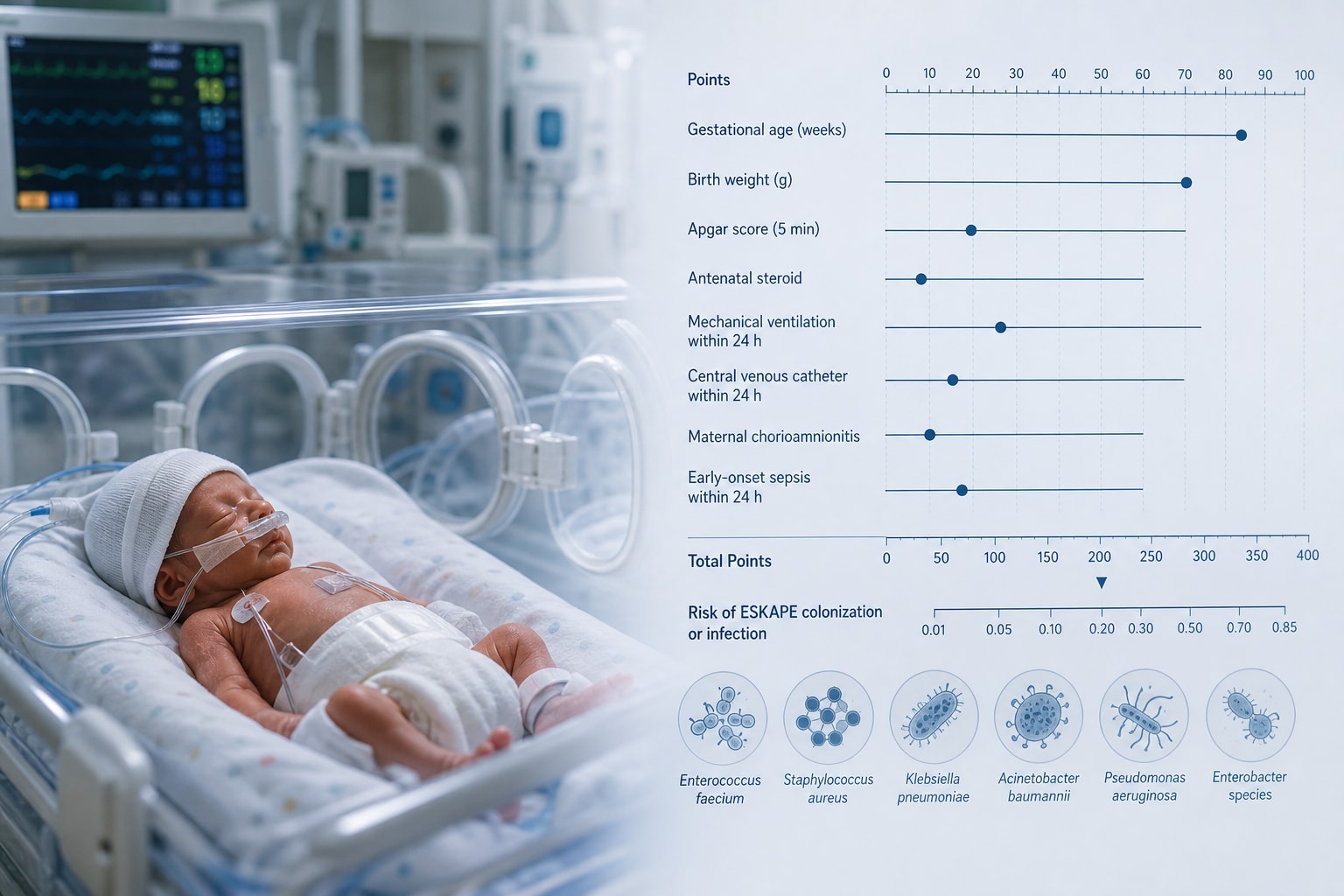
A nomogram was developed for early detection of hospital-acquired ESKAPE infections in very preterm infants, utilizing clinical indicators available within the first 24 hours after birth. The model demonstrated moderate discrimination and good calibration, supporting early risk stratification in NICUs.
Background
ESKAPE pathogens are significant contributors to hospital-acquired infections in very preterm infants, who are particularly vulnerable due to their immature immune systems and frequent medical interventions. Early identification of infants at high risk for ESKAPE colonization or infection is crucial for implementing timely infection control measures and improving clinical outcomes. This study addresses the urgent need for effective predictive tools in neonatal intensive care settings.
Data Highlights
{'validation_cohort': {'Infants with ESKAPE infection': 'Not specified'}}
Key Findings
16.56% of very preterm infants developed hospital-acquired ESKAPE colonization or infection.
67.5% of infections were identified within 14 days after birth.
The four predictors retained in the nomogram were GA at birth, initial invasive mechanical ventilation, vasoactive exposure within the first 24 hours, and 5-minute Apgar score.
The nomogram showed moderate discrimination with AUC values of 0.786 and 0.770 in training and validation cohorts, respectively.
Calibration curves indicated good agreement between predicted probabilities and observed risks.
Clinical Implications
The developed nomogram can assist healthcare professionals in identifying very preterm infants at high risk for ESKAPE infections, enabling targeted infection control strategies. Early risk stratification may lead to improved clinical management and outcomes in NICU settings. Further validation and prospective studies are necessary for routine clinical application.
Conclusion
This study presents a valuable tool for early prediction of hospital-acquired ESKAPE infections in very preterm infants. Future research should focus on external validation and implementation in clinical practice.