EUS-guided hepaticogastrostomy versus EUS-guided hepaticogastrostomy with antegrade stent placement in patients with unresectable malignant distal biliary obstruction: a meta-analysis of individual patient data - Report - MDSpire
Advertisement
EUS-guided hepaticogastrostomy versus EUS-guided hepaticogastrostomy with antegrade stent placement in patients with unresectable malignant distal biliary obstruction: a meta-analysis of individual patient data
Clinical Report: Comparative Analysis of EUS-Guided Hepaticogastrostomy Techniques
Overview
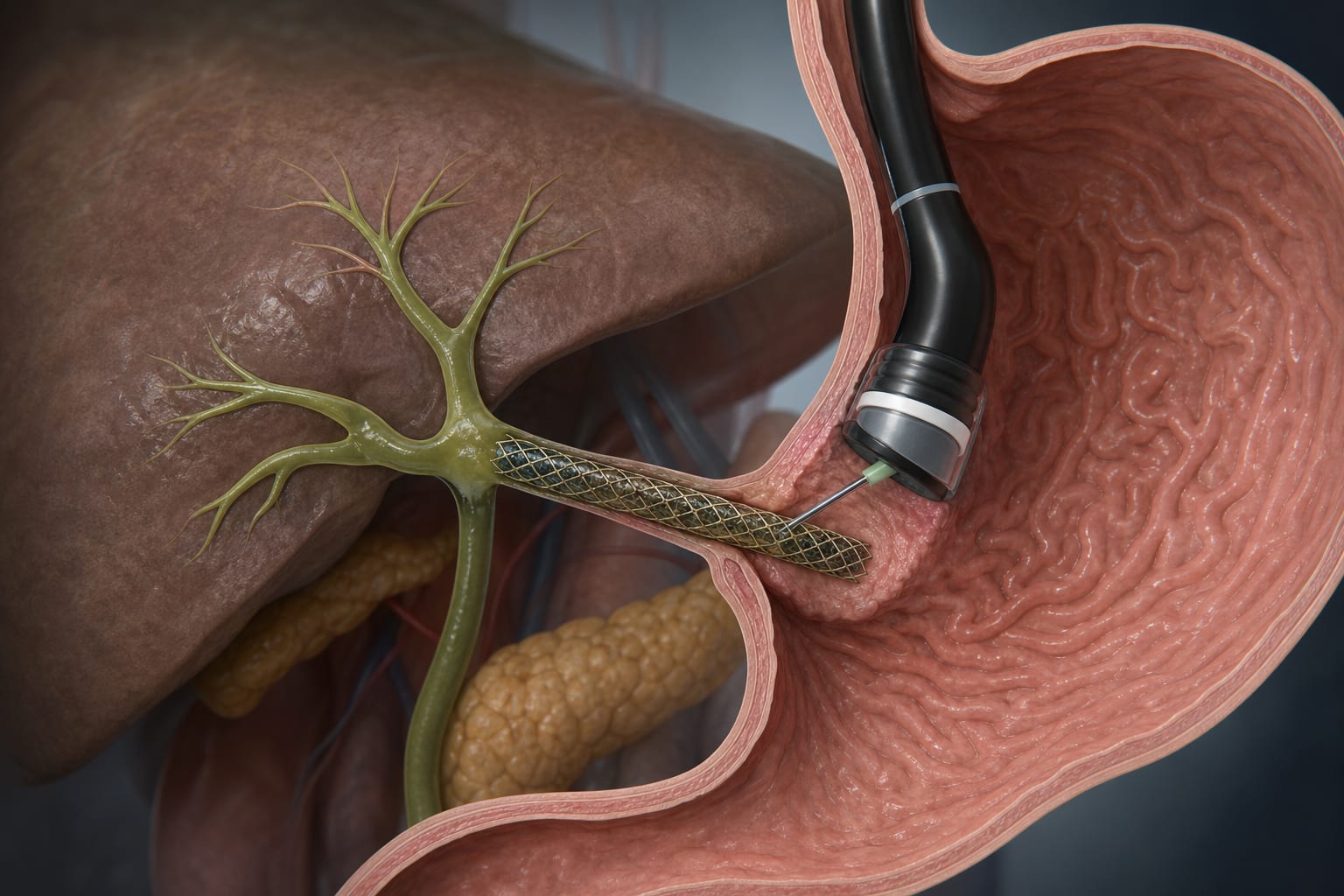
This meta-analysis compares the efficacy and safety of EUS-guided hepaticogastrostomy (HGS) alone versus EUS-guided hepaticogastrostomy with antegrade stenting (HGAS) in patients with unresectable malignant distal biliary obstruction.
Background
Malignant biliary obstruction (MBO) poses significant challenges in management, particularly in patients with pancreatic cancer. Traditional biliary drainage methods, such as ERCP, may fail in certain cases, necessitating alternative approaches like EUS-guided biliary drainage (EUS-BD). Understanding the comparative effectiveness of EUS-HGS and HGAS is crucial for optimizing patient outcomes.
Data Highlights
No numerical data was provided in the source material.
Key Findings
EUS-HGS is a standard procedure for biliary drainage in cases where ERCP fails.
HGAS combines antegrade stenting with HGS, potentially offering two drainage routes.
Recurrent biliary obstruction (RBO) is a major complication associated with HGS and AGS.
The study adhered to PRISMA guidelines and included both RCTs and observational studies.
Quality assessment of studies was performed using the Newcastle-Ottawa Scale.
Clinical Implications
The findings suggest that HGAS may be a more effective option for patients with unresectable MBO, potentially reducing the incidence of recurrent biliary obstruction. Clinicians should consider this technique when managing patients who have failed ERCP.
Conclusion
The comparative analysis highlights the potential benefits of HGAS over HGS alone in managing malignant biliary obstruction, warranting further investigation in clinical practice.