Endoscopic mucosal resection versus endoscopic submucosal dissection for early colorectal cancer and precursor lesions: a retrospective study - Report - MDSpire
Advertisement
Endoscopic mucosal resection versus endoscopic submucosal dissection for early colorectal cancer and precursor lesions: a retrospective study
Comparative Analysis of EMR and ESD for Early Colorectal Cancer
Overview
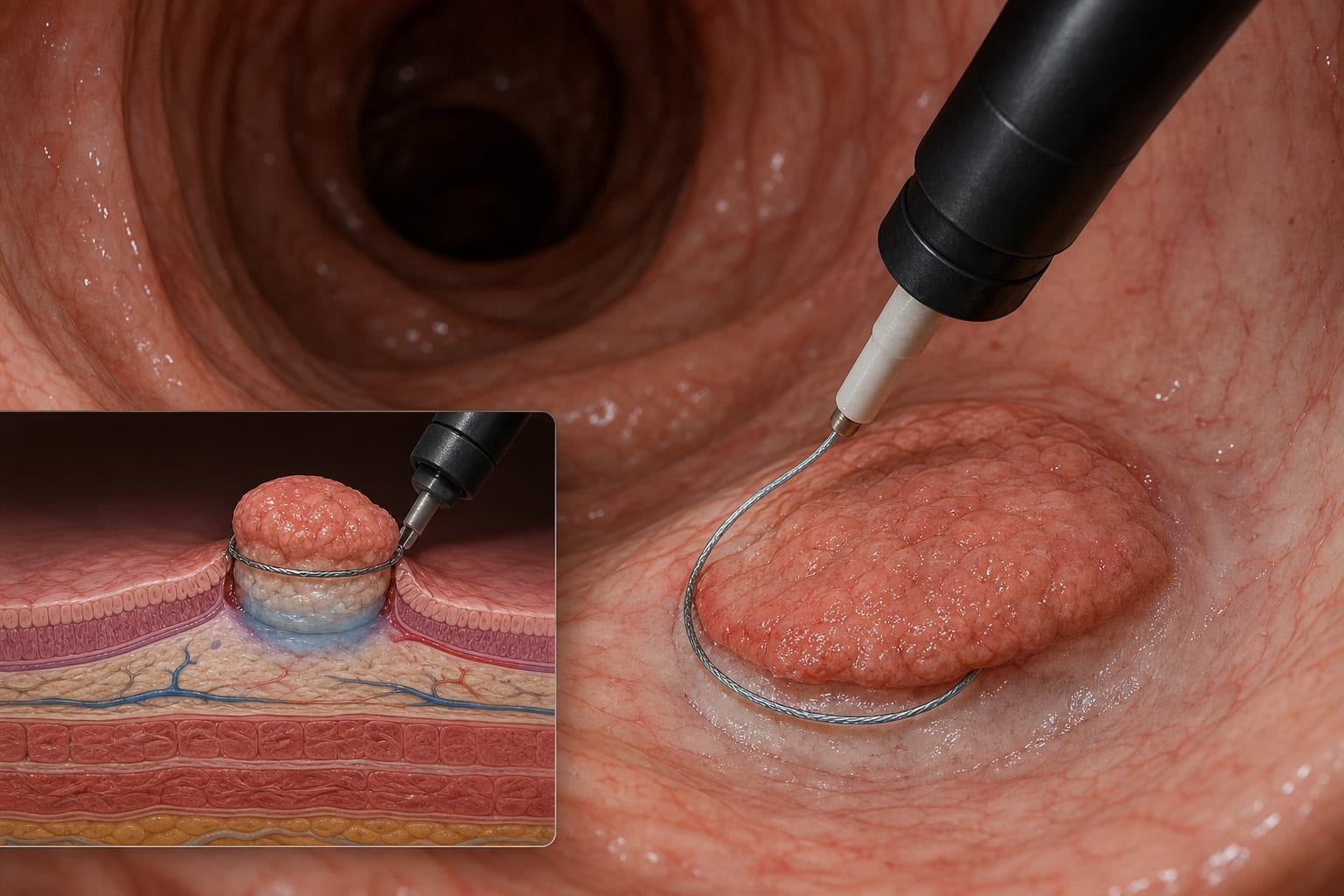
This study compares the efficacy and safety of endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) for early colorectal cancer and precursor lesions. ESD demonstrated superior resection rates for lesions ≥20 mm, particularly those ≥30 mm, but with higher complication rates in the right colon.
Background
Colorectal cancer (CRC) is a leading cause of cancer-related mortality. Endoscopic resection techniques, including EMR and ESD, are standard treatments for early CRC and precursor lesions.
Data Highlights
Lesion Size
Procedure
En Bloc Resection Rate
Complete Resection Rate
Curative Resection Rate
Complication Rate
>=20 mm
ESD
91.2%
85.3%
82.4%
40.0% (right colon)
>=20 mm
EMR
71.4%
62.9%
60.0%
6.3% (right colon)
<20 mm
EMR
—
—
—
—
Key Findings
ESD achieved higher en bloc resection rates for lesions ≥20 mm compared to EMR (91.2% vs. 71.4%, p = 0.036).
For lesions ≥30 mm, ESD showed significantly better complete (85.3% vs. 62.9%, p = 0.034) and curative resection rates (82.4% vs. 60.0%, p = 0.041) than EMR.
Complication rates were significantly higher for right-colon ESD compared to EMR (40.0% vs. 6.3%, p = 0.046).
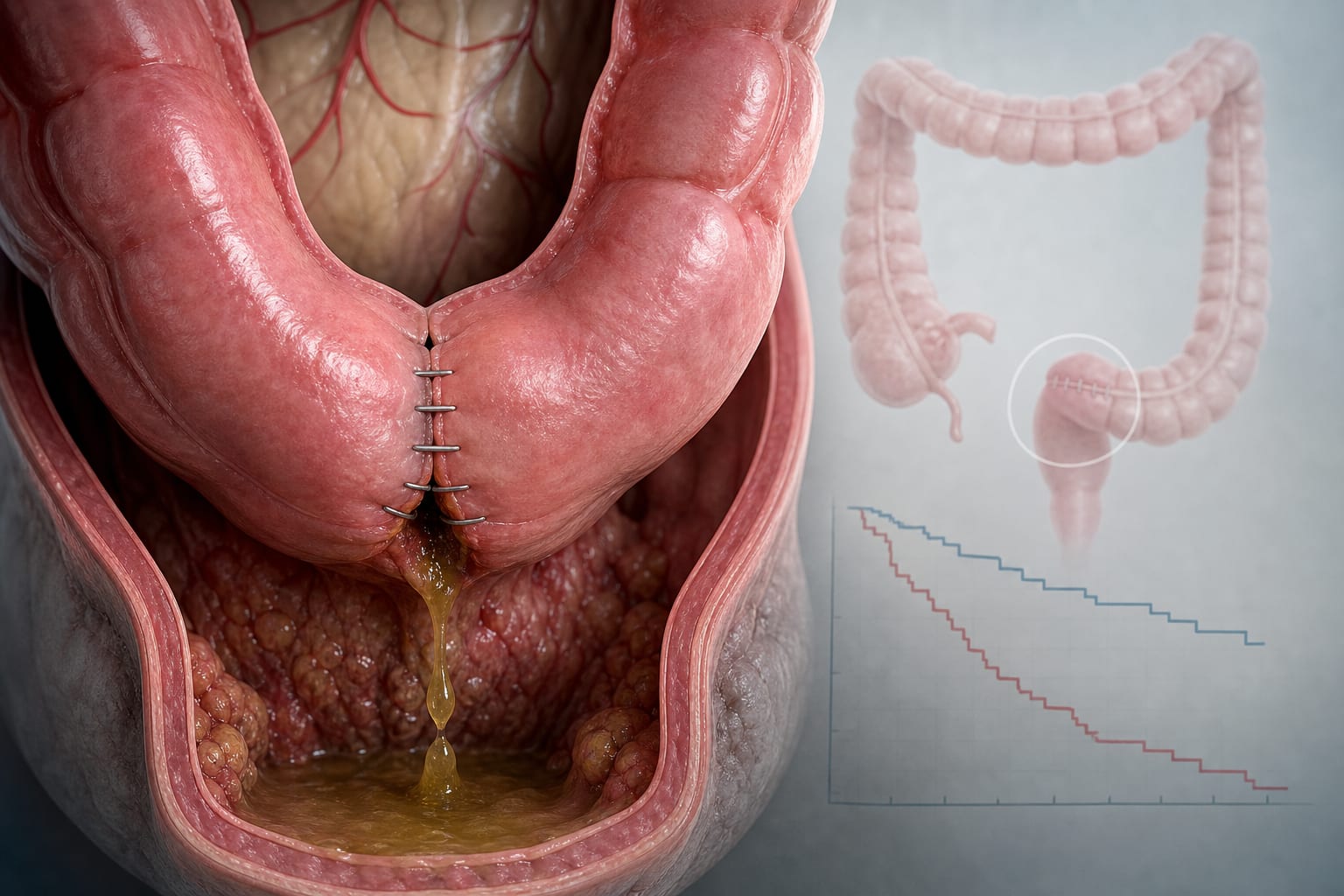
At 12-month follow-up, recurrence rates were lower for ESD (2.1%) compared to EMR (11.3%), though not statistically significant (p = 0.072).
Multivariable analysis identified ESD as an independent predictor of en bloc resection (OR 3.85, 95% CI 1.42–10.43, p = 0.008).
Clinical Implications
For lesions ≥20 mm, ESD is recommended due to its superior resection outcomes, especially for larger lesions. EMR remains the preferred method for lesions <20 mm. Clinicians should consider the higher complication rates associated with ESD, particularly in the right colon.
Conclusion
ESD offers better resection outcomes for larger lesions but comes with increased complication risks. EMR is suitable for smaller lesions.