Development and internal validation of a nomogram for predicting adverse pregnancy outcomes in women with early-onset preeclampsia
-
By
-
Haiqiong Ye
-
Qinlin Zheng
-
June 17, 2026
-
0 min
Clinical Report: Predictive Nomogram for Adverse Outcomes in EOPE
Overview
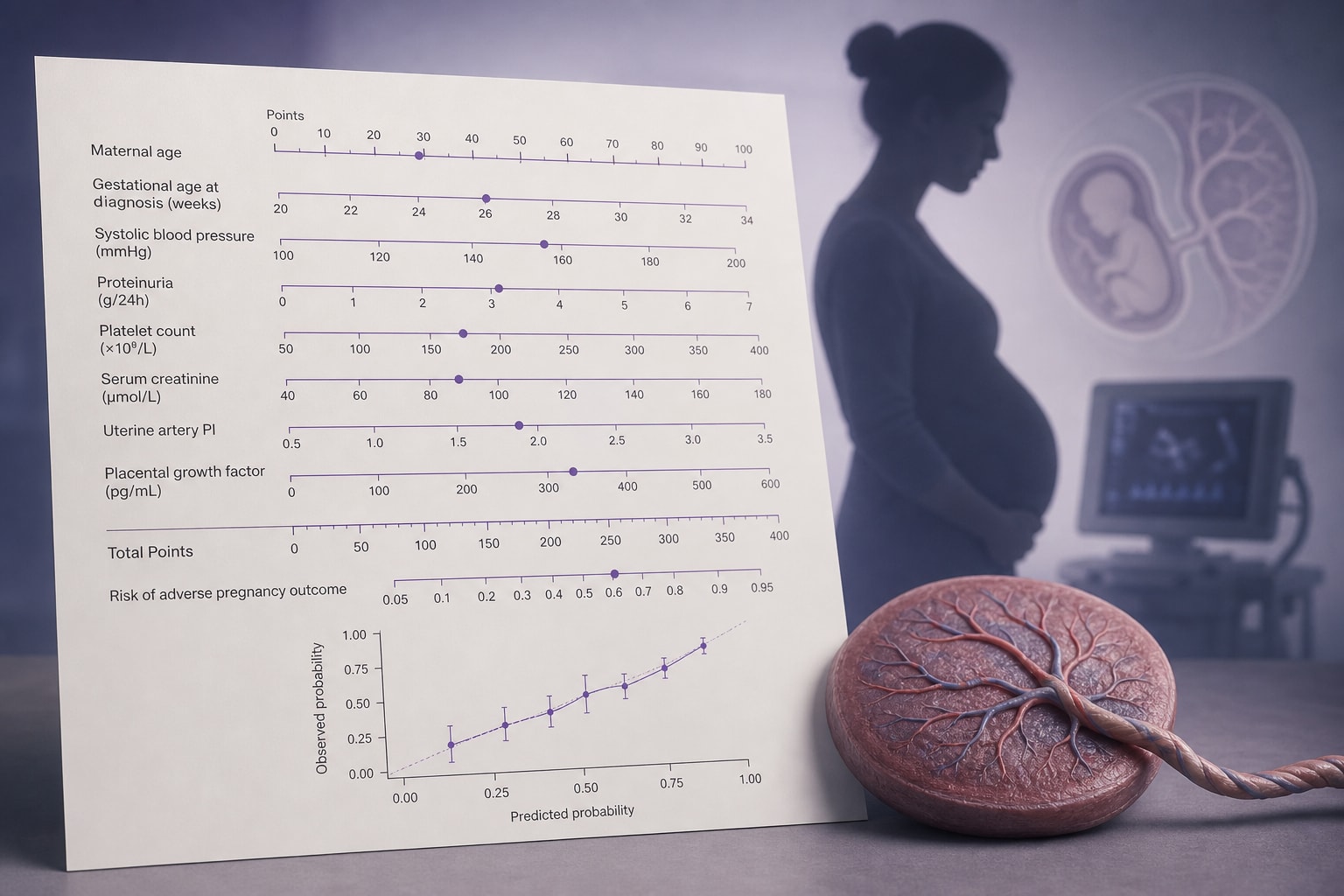
This study developed and validated a nomogram to predict adverse pregnancy outcomes in women with early-onset preeclampsia (EOPE). The model incorporates seven independent predictors and demonstrates good predictive performance, with an area under the curve (AUC) of 0.859, indicating strong discrimination ability for identifying high-risk patients.
Background
Early-onset preeclampsia (EOPE) is a serious obstetric condition that significantly increases the risk of adverse maternal and fetal outcomes. Identifying patients at high risk for these outcomes is crucial for timely clinical intervention and improved management. The development of predictive models can aid in risk stratification and guide clinical decision-making in this vulnerable population.
Data Highlights
| Predictor | Association with Risk |
|---|---|
| Gestational age at admission | Lower age increases risk |
| Systolic blood pressure | Each 10-mmHg increase increases risk |
| Urine protein score | Each 1-grade increase increases risk |
| Platelet count | Each 50 × 109/L decrease increases risk |
| AST level | Each 10-U/L increase increases risk |
| Fetal growth restriction | Associated with increased risk |
| HELLP syndrome | Associated with increased risk |
Key Findings
- Seven independent predictors were identified for adverse pregnancy outcomes in EOPE.
- The nomogram showed an AUC of 0.859 in the validation cohort.
- Calibration curves indicated acceptable agreement between predicted and observed risks.
- Decision curve analysis suggested potential clinical net benefit across relevant threshold probabilities.
- The model is intended for risk stratification after EOPE diagnosis, not for early prediction.
- External validation is necessary before clinical implementation to ensure reliability across diverse populations.
Clinical Implications
The nomogram can assist clinicians in identifying women with EOPE at higher risk for adverse outcomes, facilitating timely interventions. However, external validation is crucial before clinical implementation to ensure its reliability across diverse populations.
Conclusion
The developed nomogram provides a valuable tool for risk stratification in women diagnosed with EOPE, demonstrating good predictive performance. Further multicenter validation is essential for broader clinical application, and the proposed risk categories should not be used as definitive clinical decision cutoffs without external validation.
Related Resources & Content
- BMC Pregnancy and Childbirth, 2026 -- Development and internal validation of a predictive model for intrapartum hypertension: a retrospective case-control study
- BMC Pregnancy and Childbirth, 2026 -- The use of the first trimester (AST × LDH × urea) / (platelet × hemoglobin) index in the prediction of preeclampsia
- conexiant -- ML Model May Predict Preeclampsia Risk
- Frontiers in Medicine, 2026 -- Weighted Risk Scoring System for Predicting Peripartum Transfusion: Development and Internal Validation
- PLGF-based testing to help diagnose suspected preterm pre-eclampsia
- Predictive accuracy of sFlt-1/PlGF ratio for preeclampsia and adverse outcomes: prospective, multicenter including primary, secondary, and tertiary care institutions, observational study in Japan | Hypertension Research
- Aspirin versus Placebo in Pregnancies at High Risk for Preterm Preeclampsia | New England Journal of Medicine
- PLGF-based testing to help diagnose suspected preterm pre-eclampsia
- Predictive accuracy of sFlt-1/PlGF ratio for preeclampsia and adverse outcomes: prospective, multicenter including primary, secondary, and tertiary care institutions, observational study in Japan | Hypertension Research
- Aspirin versus Placebo in Pregnancies at High Risk for Preterm Preeclampsia | New England Journal of Medicine
This content is an AI-generated, fully rewritten summary based on a published scholarly article. It does not reproduce the original text and is not a substitute for the original publication. Readers are encouraged to consult the source for full context, data, and methodology.