Case Report: A diagnostic chameleon of EBV-associated immune dysregulation: HLH unmasking multiple myeloma with subsequent emergence of aggressive B-cell lymphoma - Report - MDSpire
Advertisement
Case Report: A diagnostic chameleon of EBV-associated immune dysregulation: HLH unmasking multiple myeloma with subsequent emergence of aggressive B-cell lymphoma
Clinical Report: EBV-Related Immune Dysregulation in HLH and Lymphoma
Overview
This case study details a 70-year-old female with hemophagocytic lymphohistiocytosis (HLH) as the initial manifestation of multiple myeloma (MM). Despite achieving remission of both conditions, HLH relapsed with persistent Epstein–Barr virus (EBV) viremia, leading to the development of aggressive B-cell lymphoma.
Background
Hemophagocytic lymphohistiocytosis (HLH) is a severe hyper-inflammatory syndrome often triggered by infections, autoimmune diseases, or malignancies. The association between multiple myeloma and HLH is rare, and the emergence of distinct lymphoid neoplasms under EBV-related immune dysregulation is not well characterized. Understanding these relationships is crucial for improving diagnosis and treatment strategies.
Data Highlights
Parameter
Value
Hemoglobin
79 g/L
Platelets
40 × 10^9/L
White Blood Cell Count
2.13 × 10^9/L
Ferritin
9928 ng/mL
Soluble IL-2 Receptor (sCD25)
37587 u/mL
EBV-DNA
1.43 × 10^6 copies/mL
Key Findings
HLH was diagnosed based on the fulfillment of 5 out of 8 HLH-2004 criteria.
Multiple myeloma was established through bone marrow examination revealing increased plasma cells and cytogenetic abnormalities.
EBV viremia persisted despite treatment, indicating a complex interplay between EBV and HLH.
Anti-PD-1 therapy provided only transient control of EBV viremia.
The patient developed aggressive large B-cell lymphoma, complicating the clinical picture.
Severe chemotherapy-related myelosuppression and sepsis ultimately led to multi-organ failure and death.
Clinical Implications
This case underscores the diagnostic challenges in identifying lymphoid neoplasms in patients with EBV-associated immune dysregulation. Clinicians should be vigilant for HLH in patients with multiple myeloma and consider the potential for concurrent lymphoid malignancies. The limited efficacy of PD-1 blockade suggests the need for alternative therapeutic strategies in managing EBV-related complications.
Conclusion
The interplay between EBV, HLH, and multiple myeloma presents significant clinical challenges. This case highlights the importance of comprehensive diagnostic approaches and the need for tailored treatment strategies in complex hematological conditions.
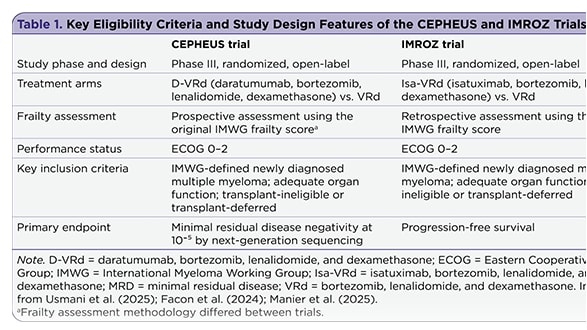
The management of newly diagnosed transplant-ineligible multiple myeloma remains challenging, in part due to the complexity of treatment decisions for frail patients. Recent subgroup analyses provide insight into whether quadruplet therapy may offer advantages over triplet therapy in this population.