High versus low ligation of the inferior mesenteric artery during transanal total mesorectal excision for low rectal cancer: impact on postoperative anastomotic leakage - Report - MDSpire
Advertisement
High versus low ligation of the inferior mesenteric artery during transanal total mesorectal excision for low rectal cancer: impact on postoperative anastomotic leakage
Comparison of High and Low Ligation Techniques of the Inferior Mesenteric Artery
Overview
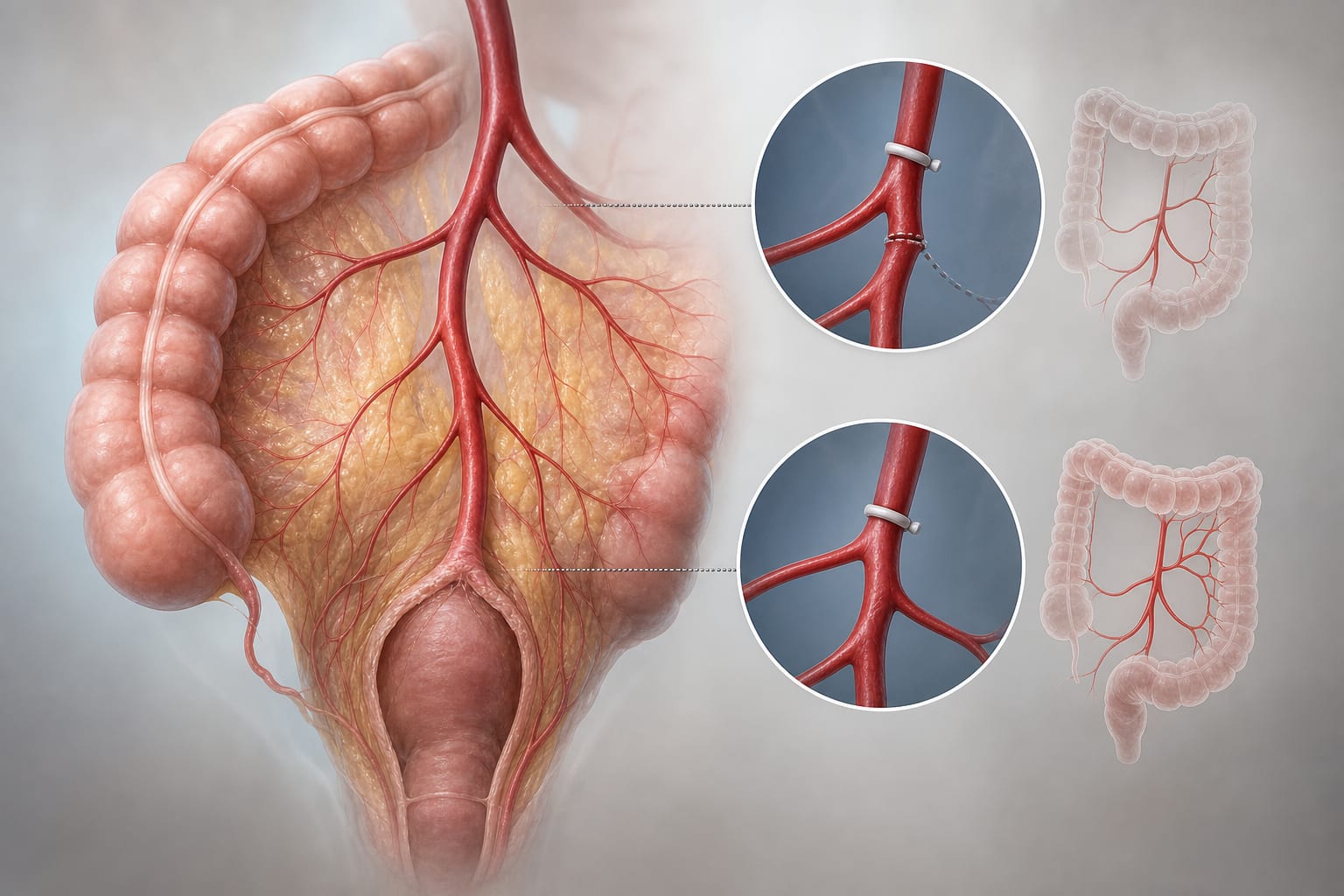
This study compares the effects of left colic artery (LCA) preservation during inferior mesenteric artery ligation on postoperative anastomotic leakage in low rectal cancer patients.
Background
Anastomotic leakage is a significant complication following rectal cancer surgery, impacting patient outcomes. The decision to preserve the left colic artery during transanal total mesorectal excision (TaTME) remains contentious, with implications for blood supply to the anastomosis. Understanding the effects of different ligation techniques on leakage rates is crucial for optimizing surgical approaches in low rectal cancer.
Data Highlights
Group
Incidence of Anastomotic Leakage
p-value
LCA Preservation (Low Ligation)
4.3%
0.036
Non-Preservation (High Ligation)
13.2%
Neoadjuvant Therapy (LCA Preservation)
7.0%
0.049
Neoadjuvant Therapy (Non-Preservation)
24.0%
Key Findings
The incidence of postoperative leakage was significantly lower in the LCA preservation group (4.3%) compared to the non-preservation group (13.2%).
Among patients who received neoadjuvant therapy, LCA preservation was associated with a lower leakage rate (7.0% vs. 24.0%).
The study involved a retrospective review of 182 patients with low rectal cancer.
Propensity score matching was used to assign patients to LCA preservation or non-preservation groups.
Clinical Implications
Surgeons may consider LCA preservation during TaTME for low rectal cancer to potentially reduce the risk of anastomotic leakage, particularly in patients undergoing neoadjuvant therapy. Individualized assessment of each patient's anatomical and pathological characteristics remains essential.
Conclusion
The study highlights the potential benefits of LCA preservation in reducing anastomotic leakage in low rectal cancer surgery, warranting further investigation in larger cohorts.