The association of remnant cholesterol inflammatory index with the risk of major adverse cardiovascular events in patients with angina undergoing percutaneous coronary intervention: a retrospective study - Report - MDSpire
Advertisement
The association of remnant cholesterol inflammatory index with the risk of major adverse cardiovascular events in patients with angina undergoing percutaneous coronary intervention: a retrospective study
Linking the Remnant Cholesterol-Inflammation Index to MACE Risk in Angina Patients
Overview
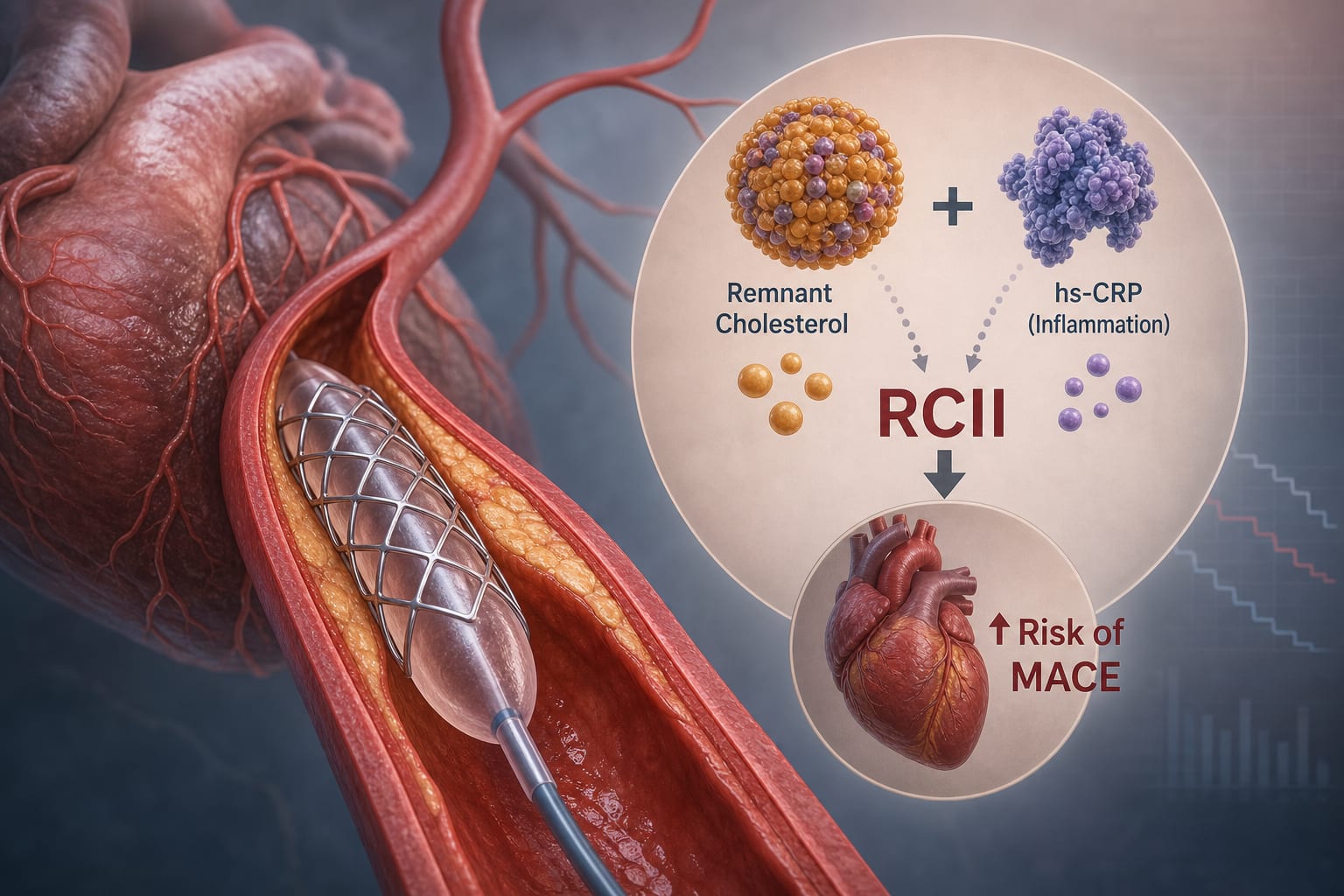
This study evaluates the association between the remnant cholesterol-inflammation index (RCII) and major adverse cardiovascular events (MACE) in angina patients undergoing percutaneous coronary intervention (PCI). Findings indicate that higher RCII correlates with increased MACE risk, suggesting its potential as a clinical biomarker.
Background
Coronary artery disease (CAD) remains a leading cause of morbidity and mortality globally, with angina being a common manifestation. Despite advancements in treatment, including PCI, patients still face significant residual cardiovascular risks. Understanding additional risk factors, such as the RCII, is crucial for improving patient outcomes post-PCI.
Data Highlights
{'format': 'Ensure the table is accessible and clearly presented.'}
Key Findings
Each standard deviation increase in RCII is associated with a 5% higher MACE risk.
Patients in the highest tertile of RCII have a significantly elevated risk of MACE compared to the lowest tertile.
RCII is significantly associated with MACE risk across various subgroups, including age, sex, and comorbidities.
RCS analysis indicates a non-linear positive association between RCII and MACE risk.
Time-dependent ROC analysis shows moderate discriminatory ability of RCII for predicting MACE.
Clinical Implications
The findings suggest that RCII could serve as a valuable biomarker for assessing MACE risk in angina patients post-PCI. Clinicians should consider incorporating RCII measurements into routine risk assessments to better identify patients at higher risk for adverse cardiovascular events.
Conclusion
The study highlights the potential of RCII as a clinical tool for predicting MACE risk in angina patients undergoing PCI, emphasizing the need for further research to validate its utility in clinical practice.