Autoimmune GFAP astrocytopathy with eosinophils on cerebrospinal fluid cytology and isolated spinal cord lesions on MRI: a case report - Report - MDSpire
Advertisement
Autoimmune GFAP astrocytopathy with eosinophils on cerebrospinal fluid cytology and isolated spinal cord lesions on MRI: a case report
Clinical Report: Eosinophilic Presence in CSF Cytology in Autoimmune GFAP Astrocytopathy
Overview
This case study highlights the presence of eosinophils in cerebrospinal fluid (CSF) cytology in a patient with autoimmune GFAP astrocytopathy, characterized by isolated spinal cord lesions on MRI. The findings suggest a distinct inflammatory profile and underscore the importance of considering this diagnosis even in the absence of brain MRI abnormalities.
Background
Autoimmune GFAP astrocytopathy is an inflammatory disorder of the central nervous system associated with GFAP-IgG, often presenting as meningoencephalitis or myelitis. Isolated spinal cord lesions without corresponding brain MRI abnormalities are rare and can complicate diagnosis. The identification of eosinophils in CSF cytology is particularly uncommon and may indicate unique inflammatory mechanisms.
Data Highlights
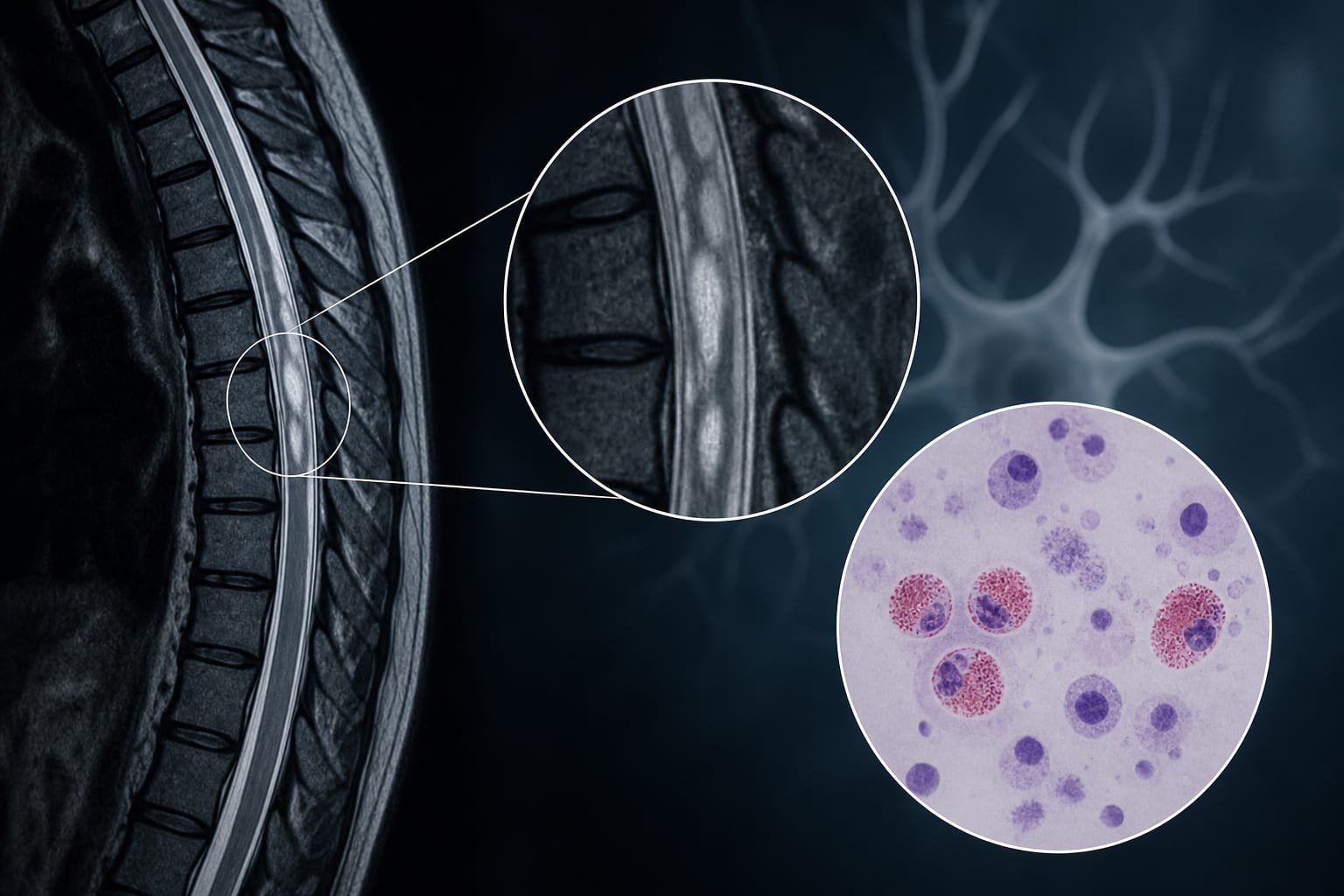
The patient presented with fever, headache, and urinary retention. MRI showed isolated thoracic spinal cord lesions, while CSF analysis revealed elevated opening pressure, pleocytosis, increased protein, and 10% eosinophils. Following treatment with high-dose intravenous methylprednisolone, there was marked clinical and radiological improvement.
Key Findings
Patient presented with fever, headache, and urinary retention.
Brain MRI was unremarkable, while spinal MRI revealed discontinuous patchy long-segment intramedullary lesions.
CSF GFAP-IgG was positive at a titer of 1:32, while serum GFAP-IgG was negative.
High-dose intravenous methylprednisolone led to significant clinical and radiological improvement.
Isolated spinal cord lesions may indicate autoimmune GFAP astrocytopathy even without brain MRI abnormalities.
Clinical Implications
Clinicians should consider autoimmune GFAP astrocytopathy in patients presenting with isolated inflammatory spinal cord lesions, particularly when CSF eosinophils are detected. Early recognition and treatment with corticosteroids may lead to significant clinical improvement.
Conclusion
This case underscores the importance of recognizing eosinophilic presence in CSF as a potential indicator of autoimmune GFAP astrocytopathy, particularly in the context of isolated spinal cord lesions.