Post-Stereotactic Radiosurgery Pituitary Hormone Dysfunction in Patients with Pituitary Adenomas
Overview
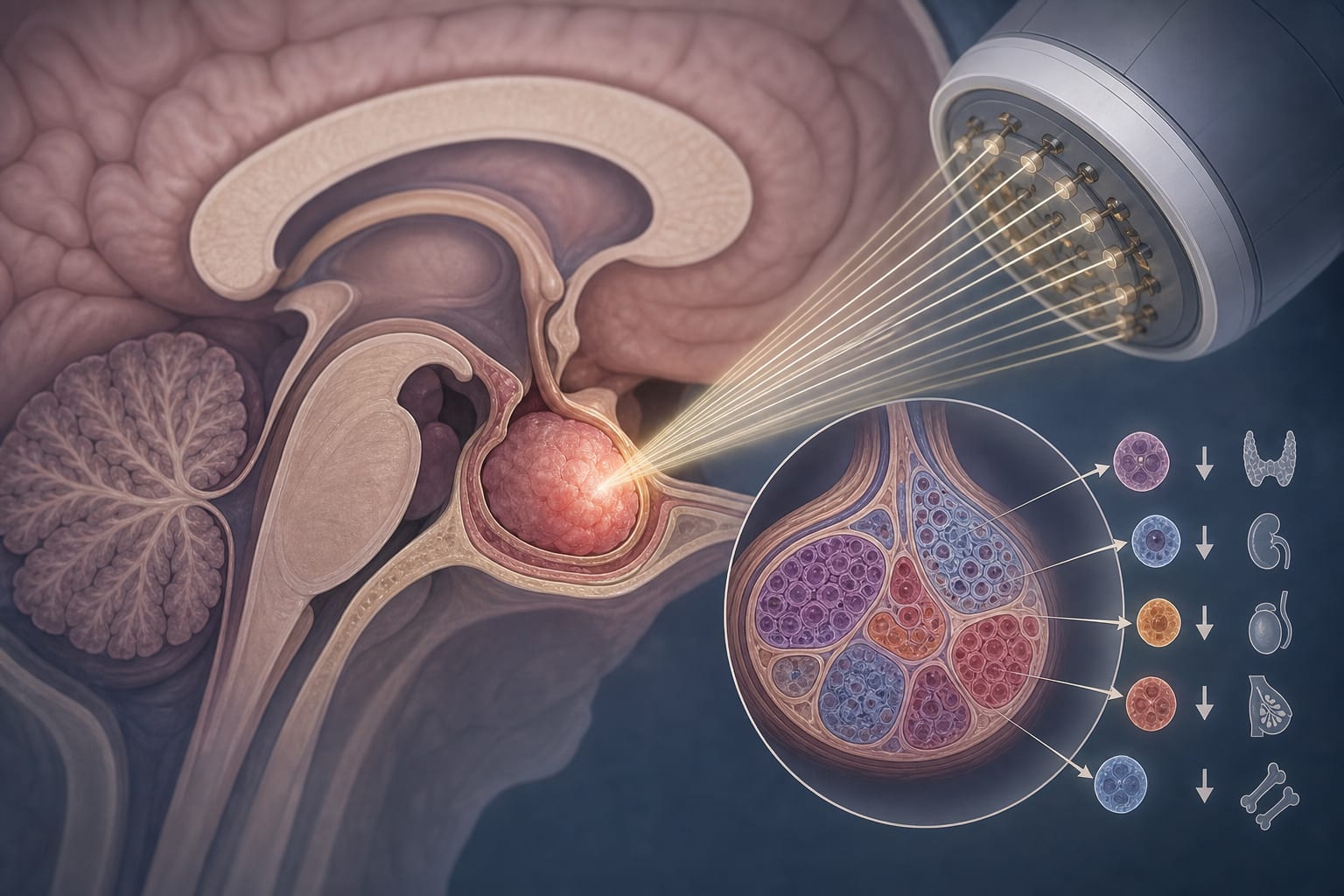
Stereotactic radiosurgery (SRS) is increasingly used to manage pituitary adenomas, but it carries a significant risk of hypopituitarism, with incidence rates ranging from 21% to 50%. Understanding the mechanisms and predictors of hormone dysfunction following SRS is crucial for optimizing patient outcomes.
Background
Pituitary adenomas account for a notable percentage of intracranial tumors and can lead to significant hormonal dysfunction. The management of these tumors often involves surgical resection and radiotherapy, with SRS emerging as a less invasive option. However, the potential for post-treatment hormonal deficiencies necessitates careful consideration of treatment strategies.
Data Highlights
No specific numerical data or trial results were provided in the source material.
Key Findings
Hypopituitarism is the most common complication of SRS, with an incidence of 21% to 50%.
Complete surgical resection is not always achievable, particularly in cases of tumor invasion.
Progression of residual tumors occurs in approximately 50% of pituitary adenomas within 10 years post-surgery.
SRS is primarily used as adjuvant therapy for residual tumors and can lead to tumor shrinkage without guaranteeing hormonal remission.
Biochemical remission criteria vary across studies, complicating comparisons of treatment efficacy.
Clinical Implications
Clinicians should be aware of the high incidence of hypopituitarism following SRS and consider the timing and extent of hormonal monitoring post-treatment. The potential for delayed hormonal deficiencies emphasizes the need for ongoing endocrine evaluation in patients treated with SRS.
Conclusion
SRS presents a valuable option for managing pituitary adenomas, but the risk of hypopituitarism necessitates a thorough understanding of its mechanisms and careful patient follow-up.