Integrated management of atrial fibrillation and comorbidities in the community: a generalist-specialist collaborative RCT and subgroup analysis - Report - MDSpire
Advertisement
Integrated management of atrial fibrillation and comorbidities in the community: a generalist-specialist collaborative RCT and subgroup analysis
Clinical Report: Collaborative Care Approach for Atrial Fibrillation
Overview
This study evaluates a community-based integrated care model for atrial fibrillation (AF) that emphasizes collaboration between general practitioners and specialists. Results indicate improvements in risk factor control, cardiac function, and a reduction in major adverse cardiovascular events over a 12-month period.
Background
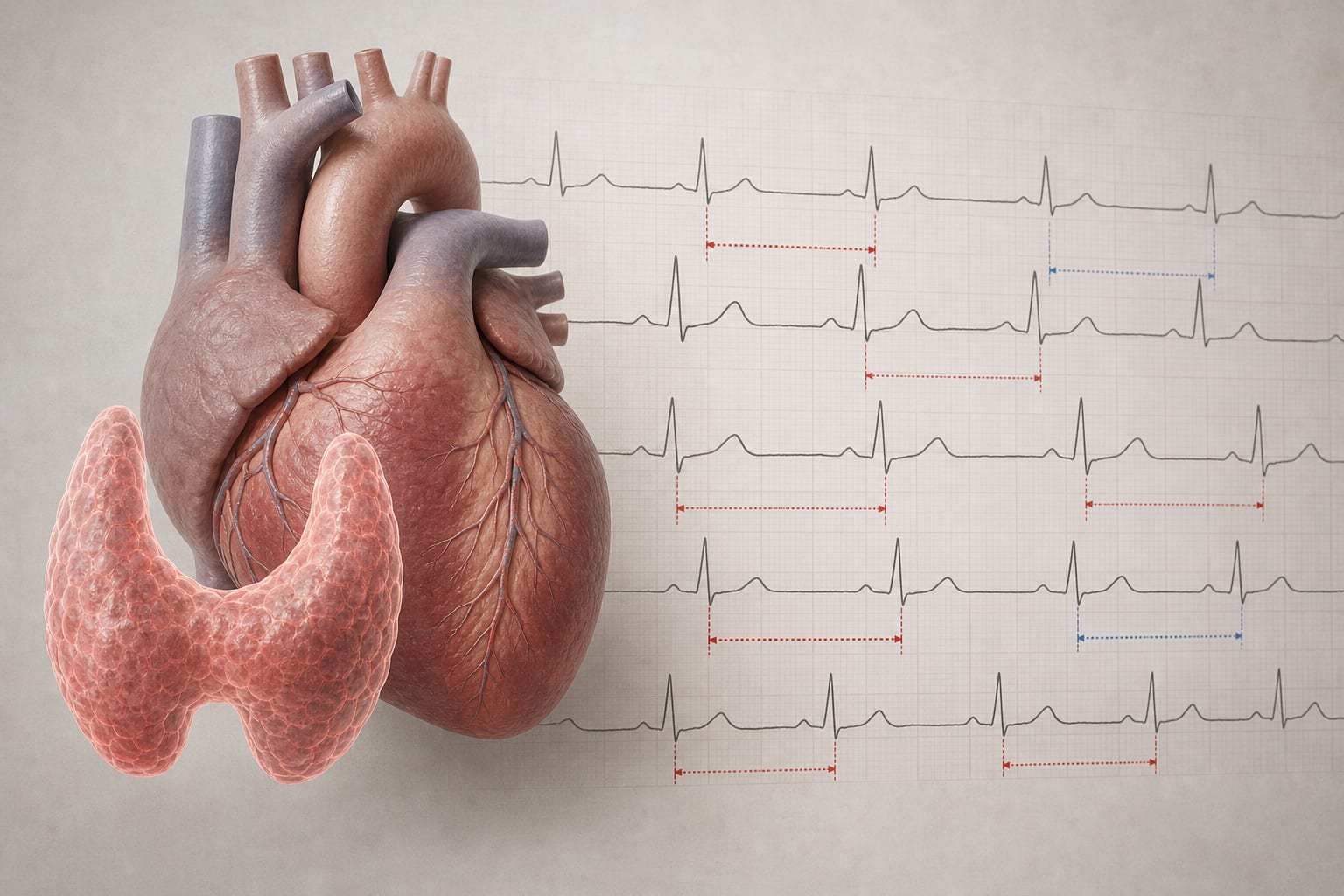
Atrial fibrillation (AF) is a leading cause of cardiogenic stroke, with a high prevalence in aging populations. In China, the burden of AF is expected to rise significantly, necessitating effective management strategies. Current fragmented care models contribute to inadequate risk factor control and increased stroke risk, highlighting the need for integrated, patient-centered approaches. Specific studies indicate that AF prevalence increases with age, and the associated stroke risk is significant.
Data Highlights
Outcome
Intervention Group
Control Group
Attainment Rates for BMI, BP, and Blood Glucose
Higher attainment rates
Lower attainment rates
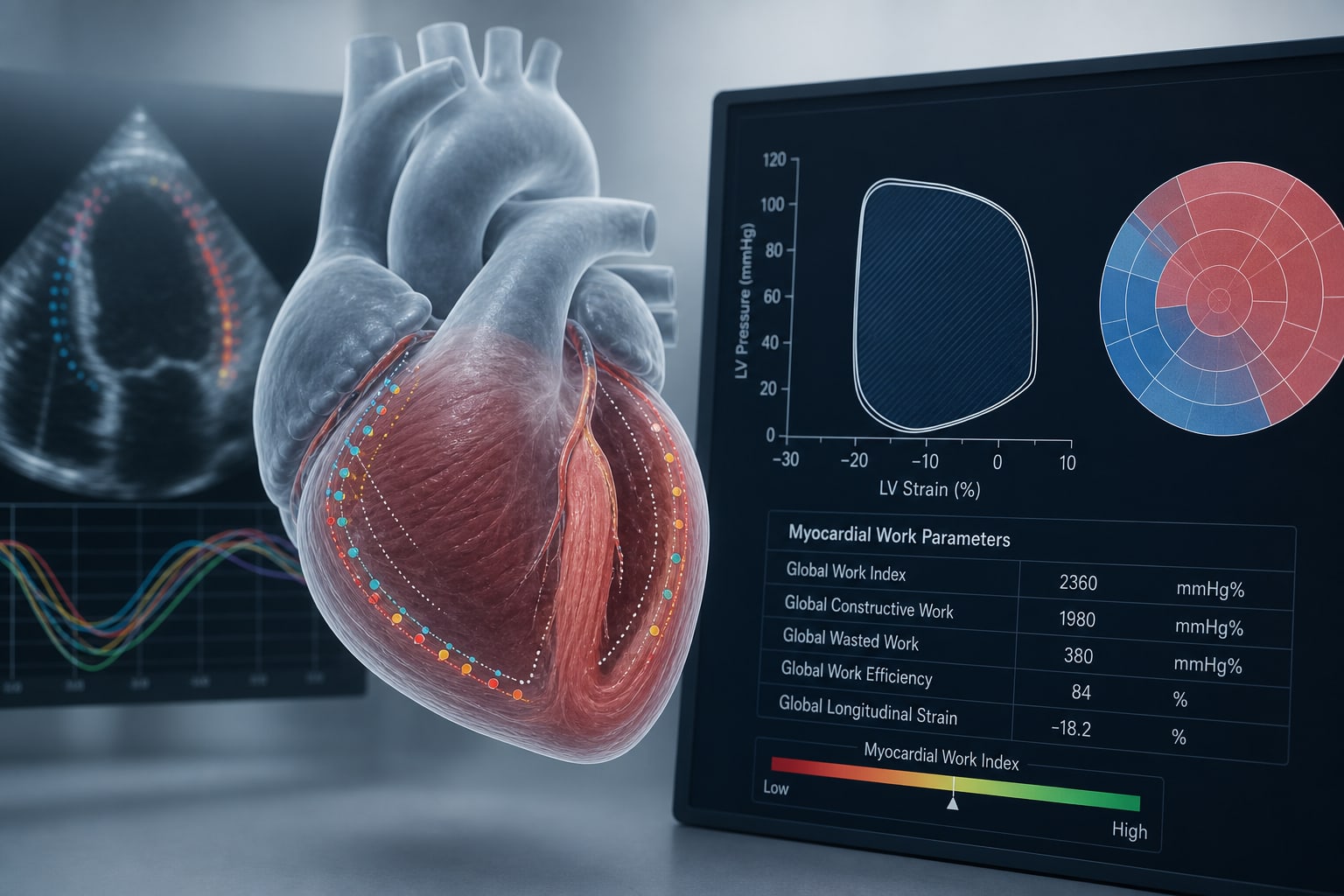
LVEF Improvement
Significant improvement
No significant change
NT-proBNP Levels
No significant difference
No significant difference
Standardized Medication Use
Higher usage rates
Lower usage rates
Composite Outcome (Heart Failure or Stroke)
Lower incidence
Higher incidence
Key Findings
The intervention group achieved higher rates of control for BMI, blood pressure, and blood glucose.
Left ventricular ejection fraction (LVEF) improved in the intervention group.
No significant difference was found in NT-proBNP levels between the two groups.
Standardized usage rates for anticoagulants and heart rate control medications were higher in the intervention group.
The incidence of the composite outcome (heart failure or stroke) was lower in the intervention group.
Subgroup analyses showed no significant interactions for age, sex, or CHA2DS2-VASc score.
Clinical Implications
Healthcare providers should consider integrated approaches that involve both generalists and specialists to improve risk factor control and reduce adverse cardiovascular events.
Conclusion
The collaborative integrated care model for AF improves patient outcomes. This approach is based on the study's findings.