Efficacy analysis of microvascular decompression and percutaneous balloon compression for trigeminal neuralgia secondary to vertebrobasilar dolichoectasia: a retrospective cohort study - Report - MDSpire
Advertisement
Efficacy analysis of microvascular decompression and percutaneous balloon compression for trigeminal neuralgia secondary to vertebrobasilar dolichoectasia: a retrospective cohort study
Comparative Effectiveness of MVD versus PBC for VBD-Associated Trigeminal Neuralgia
Overview
This retrospective cohort study compares microvascular decompression (MVD) and percutaneous balloon compression (PBC) in treating trigeminal neuralgia caused by vertebrobasilar dolichoectasia (VBD-TN). The analysis evaluates efficacy, safety, and postoperative outcomes to guide surgical decision-making in this rare TN subtype.
Background
Trigeminal neuralgia (TN) is often caused by vascular compression of the trigeminal nerve root. Vertebrobasilar dolichoectasia (VBD), characterized by elongation and tortuosity of vertebrobasilar arteries, can compress the trigeminal nerve leading to VBD-TN, a rare form accounting for 2% to 7.7% of TN cases. Microvascular decompression (MVD) is the preferred surgical treatment for classical TN but is technically challenging in VBD-TN due to the complex vascular anatomy. Percutaneous balloon compression (PBC) offers a minimally invasive alternative with simpler procedural complexity, yet comparative data on these techniques for VBD-TN remain limited.
Data Highlights
The study included patients diagnosed with VBD-TN who underwent either MVD or PBC between 2013 and 2022. Surgical selection was based on contraindications, patient preference, and tolerance for postoperative numbness. Both procedures were performed by the same experienced surgeon. Follow-up assessments occurred at 1, 6, and 12 months postoperatively, then annually, evaluating pain relief and complications using the Barrow Neurological Institute scoring system.
Key Findings
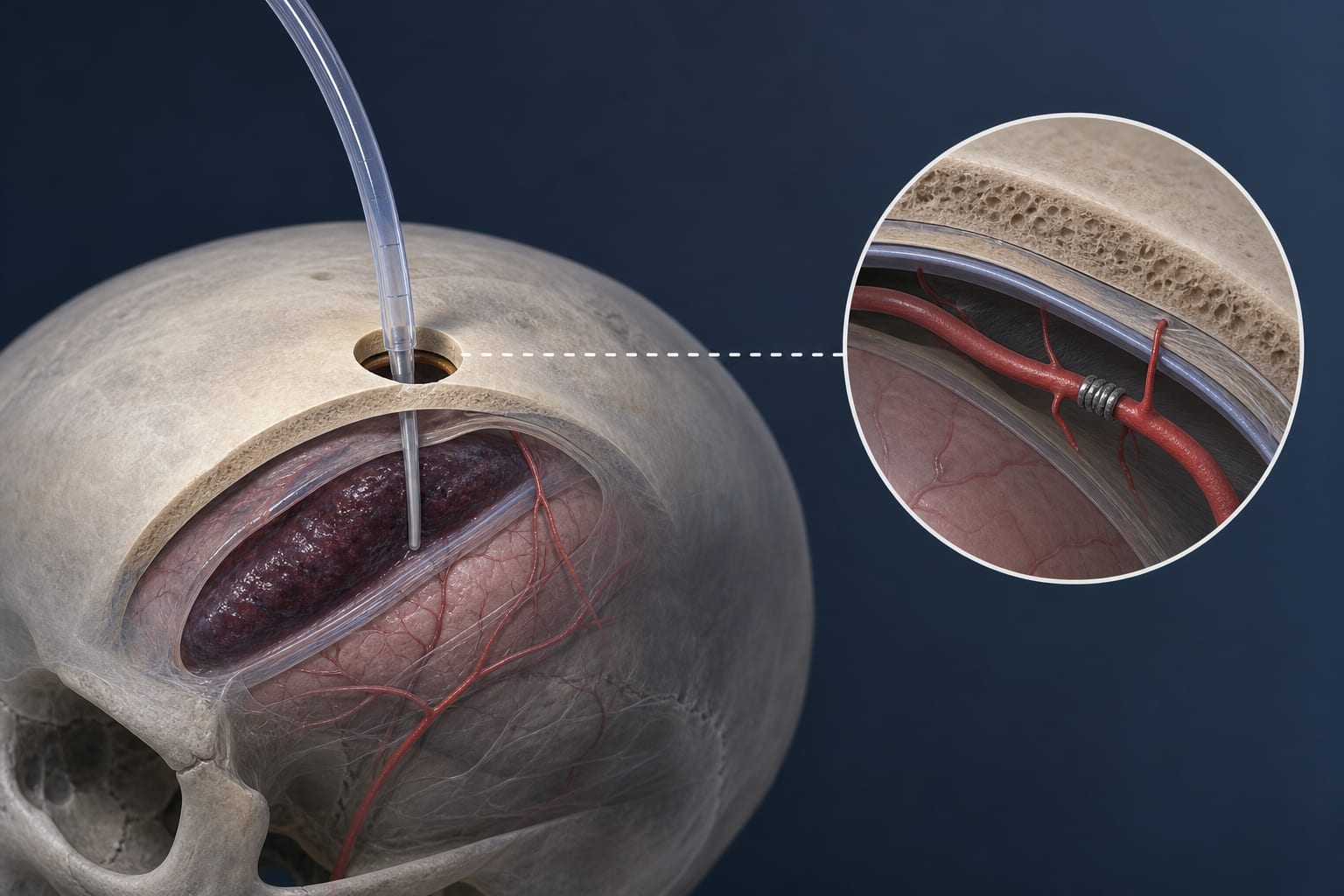
MVD involves a retrosigmoid craniotomy with microscope-endoscope assistance to place Teflon pledgets between the vertebrobasilar artery and trigeminal nerve, with selective partial posterior rhizotomy if decompression is difficult.
PBC is performed percutaneously via the foramen ovale under imaging guidance, inflating a balloon in Meckel’s cave to compress the trigeminal ganglion for 120–180 seconds.
Surgical selection depends on contraindications and patient preferences, balancing risks of craniotomy and tolerance for postoperative numbness.
Postoperative complications monitored include intracranial infection, cerebrospinal fluid leakage, facial numbness, and other cranial nerve deficits.
Follow-up data collection includes pain relief levels and adverse events to compare efficacy and safety profiles of MVD versus PBC in VBD-TN.
Clinical Implications
Clinicians should consider patient-specific factors such as contraindications, surgical risk tolerance, and expected postoperative sensory changes when selecting between MVD and PBC for VBD-TN. MVD offers direct neurovascular decompression but with higher technical complexity, while PBC provides a less invasive option with simpler procedural demands. Comprehensive preoperative imaging and multidisciplinary evaluation are essential to optimize outcomes.
Conclusion
This study provides valuable comparative insights into MVD and PBC for managing VBD-associated trigeminal neuralgia, highlighting the importance of individualized surgical planning to balance efficacy and safety. Further prospective studies are warranted to refine treatment algorithms for this rare TN subtype.
References
Article Source 2024 -- Comparative Effectiveness of Microvascular Decompression versus Percutaneous Balloon Compression for Trigeminal Neuralgia Associated with Vertebrobasilar Dolichoectasia