Clinical Report: Systematic Review and Meta-Analysis of VTE Risk Models in Lung Cancer
Overview
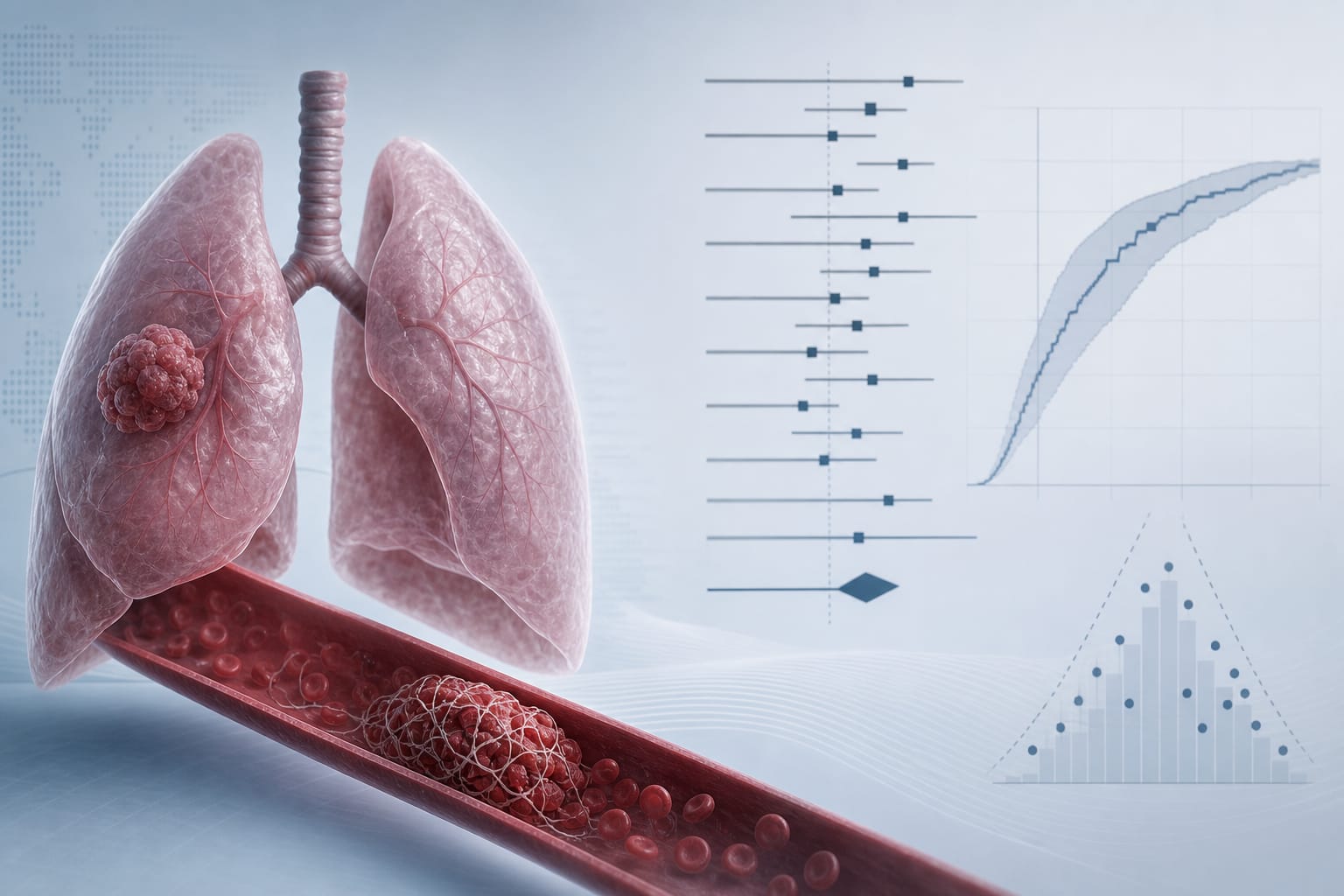
This systematic review and meta-analysis evaluated postoperative venous thromboembolism (VTE) risk prediction models in lung cancer patients. Despite identifying several models with varying predictive abilities, all studies exhibited high bias risk, limiting their clinical applicability.
Background
Lung cancer is a leading cause of cancer-related mortality, with venous thromboembolism (VTE) being a significant postoperative complication. The incidence of VTE after lung cancer surgery varies widely, influenced by multiple factors, including patient characteristics and surgical practices. Reliable risk prediction models are essential for timely thromboprophylaxis and monitoring, yet current models lack sufficient validation and methodological rigor.
Data Highlights
Model
AUC
Risk of Bias
Various Models
0.66 - 0.99
High
Pooled Model
0.85 (95% CI: 0.78–0.93)
High
Key Findings
Twenty studies involving 20 prediction models were included in the analysis.
All studies were retrospective and single-center, with high risk of bias as per PROBAST.
Logistic regression was the predominant modeling approach, with limited use of machine learning methods.
The most common predictors included D-dimer and age.
AUC values for model discrimination ranged from 0.66 to 0.99, with a pooled AUC of 0.85.
Substantial heterogeneity was observed among the models (I² = 89.1%).
Clinical Implications
Clinicians should exercise caution when using existing VTE risk prediction models for lung cancer patients due to their high risk of bias and limited applicability. Future models should focus on rigorous methodologies and multicenter validations to enhance their reliability and clinical utility.
Conclusion
The current evidence does not support the routine clinical use of existing postoperative VTE prediction models in lung cancer patients. Enhanced methodological frameworks are necessary for future studies to improve prediction accuracy.