Clinical Report: Inflammatory Remodeling and Mucus Secretion Deficiency in IBD
Overview
Revise to clarify the distinction between inflammatory remodeling and primary secretory failure.
Background
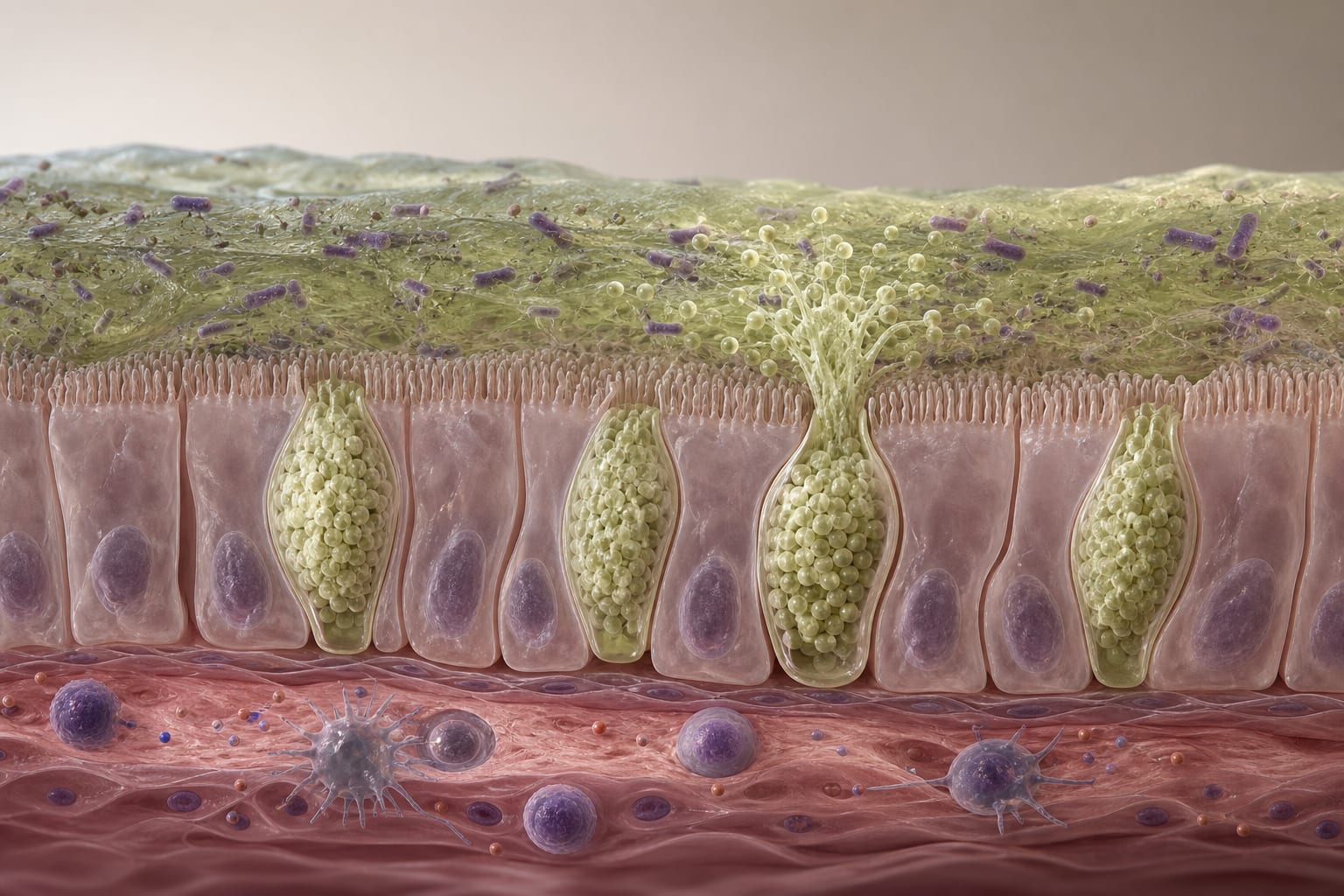
Inflammatory bowel disease (IBD) encompasses chronic conditions like Crohn's disease (CD) and ulcerative colitis (UC), characterized by immune dysregulation and epithelial barrier dysfunction. The integrity of the intestinal mucus layer is crucial for maintaining gut homeostasis, and its disruption can lead to increased exposure to luminal antigens, exacerbating inflammation. Understanding the mechanisms behind mucus dysfunction is essential for developing targeted therapies that address the root causes of IBD.
Data Highlights
Condition
Differentially Expressed Genes
Crohn's Disease
3,129
Ulcerative Colitis
3,729
Key Findings
3,129 genes were differentially expressed in Crohn's disease, and 3,729 in ulcerative colitis.
Both conditions showed upregulation of pathways related to goblet-cell differentiation and mucin transcription.
MUC1, MUC4, MUC5AC, and MUC5B were consistently upregulated in active IBD.
ER stress components, including HSPA5 and XBP1, were elevated in IBD compared to healthy controls.
Inflammatory remodeling rather than primary secretory failure is implicated in mucus barrier dysfunction in IBD.
Clinical Implications
The findings emphasize the need for therapies that target the epithelial barrier and mucus secretion processes in IBD. Clinicians should consider the role of inflammatory remodeling in treatment strategies, potentially shifting focus from solely immune modulation to include mucosal barrier restoration.
Conclusion
This study underscores the complexity of mucus dysfunction in IBD, revealing that inflammatory remodeling plays a significant role in altering mucus barrier integrity. Future therapeutic approaches should aim to address these upstream mechanisms to improve patient outcomes.