Hospital Readmissions and Long-Term Mortality in Pediatric Patients with Congenital Diaphragmatic Hernia
Overview
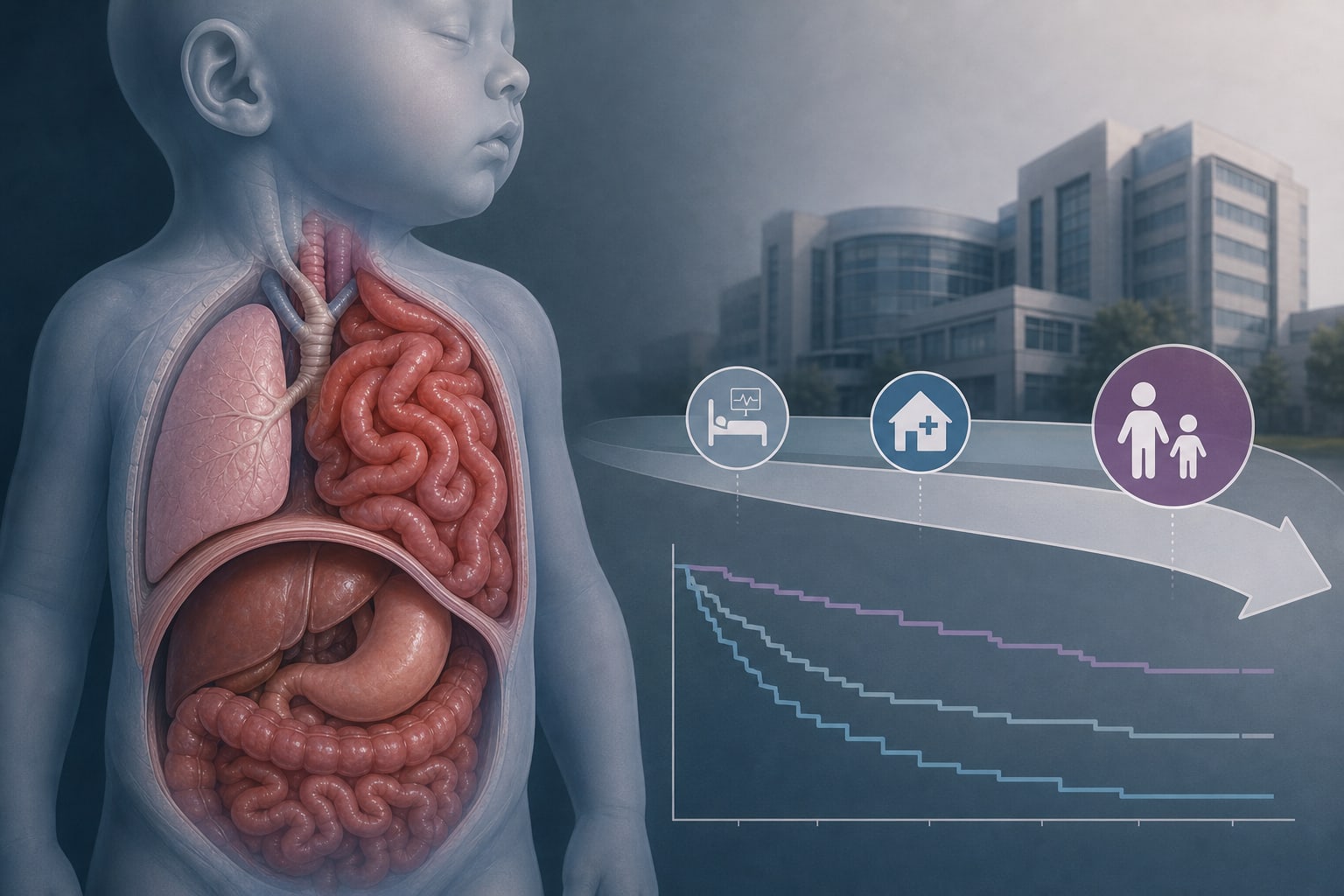
This study investigates the incidence and causes of hospital readmissions within three years for pediatric patients with congenital diaphragmatic hernia (CDH) who survived neonatal care and surgery. It also assesses late mortality and associated factors.
Background
Congenital diaphragmatic hernia (CDH) is a significant congenital anomaly affecting respiratory function and is associated with high early mortality rates. Despite improvements in survival due to standardized management, long-term outcomes, including readmission rates and late mortality, remain inadequately characterized.
Data Highlights
No numerical or trial data provided in the source material.
Key Findings
The study utilized a retrospective nationwide cohort design over 12 years using linked national health data.
Readmissions were categorized into five causes: respiratory/infectious, cardiovascular, nutritional/gastrointestinal, surgical complications, and other causes unrelated to CDH.
Individual characteristics related to CDH severity were collected, including gestational age, birth weight, and associated congenital anomalies.
Follow-up continued until May 31, 2024, or death, allowing for comprehensive assessment of outcomes.
Readmissions contribute to higher healthcare costs and prolonged hospital stays.
Clinical Implications
Healthcare providers should be aware of the high risk of readmissions in pediatric CDH patients and the associated healthcare costs. Enhanced follow-up care and monitoring may be necessary to address the complexities of this patient population.
Conclusion
Understanding readmission patterns and late mortality in pediatric patients with CDH is important for improving long-term care strategies.
Federal prosecutors allege that a Florida physician and research staff fabricated clinical trial records that were submitted into database systems used to evaluate investigational drugs.