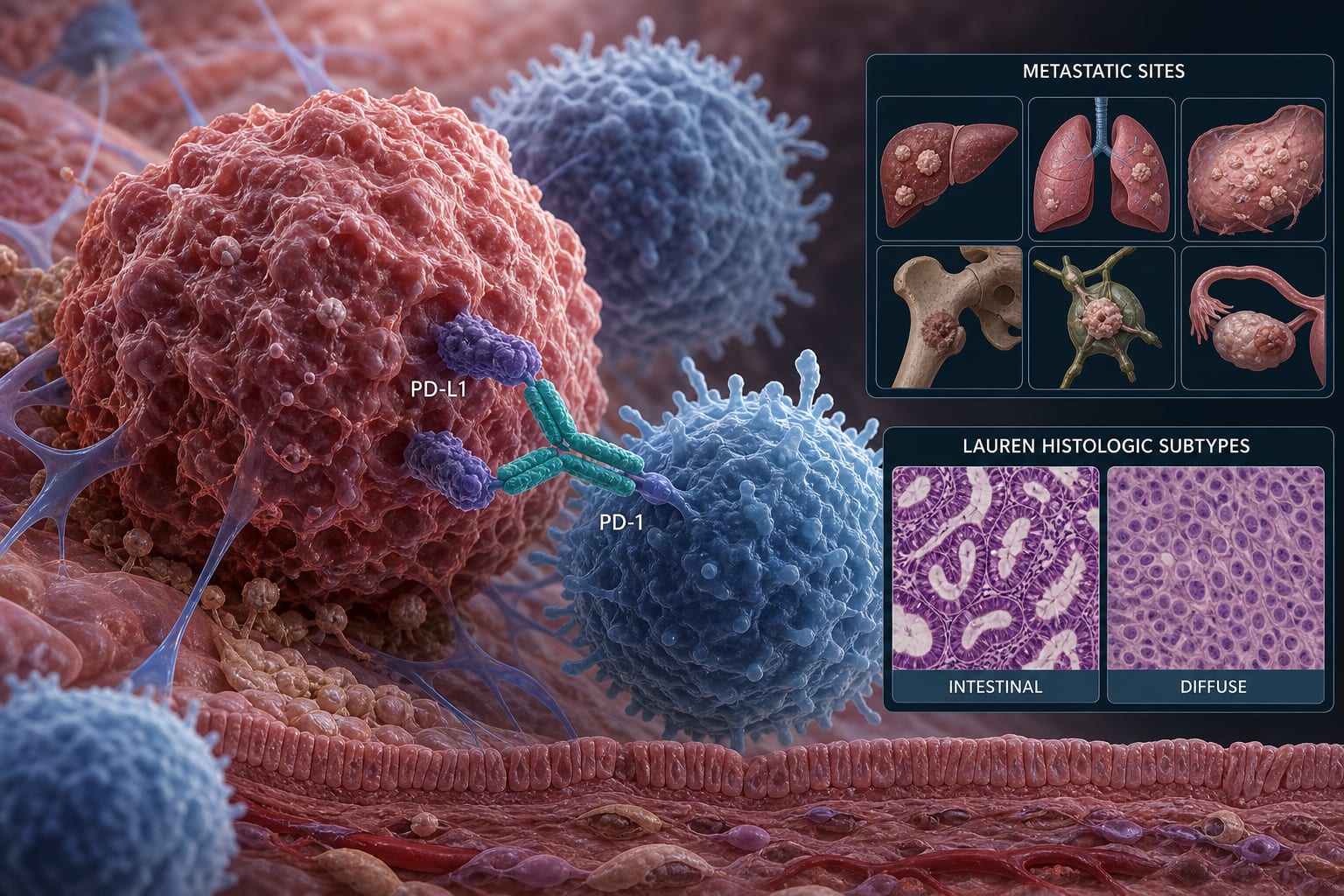
Impact of metastatic pattern and histologic subtype on PD-(L)1 inhibitor efficacy in HER2-negative advanced gastric and gastroesophageal cancer: a meta-analysis
-
By
-
Derek Tai
-
Kyung-il Kim
-
Pranati Shah
-
Daniel Park
-
Lucas Kim
-
Jianan Li
-
Claire Jung
-
Sofia Guzman
-
Gagandeep Brar
-
Shengyang Wu
-
Dani Castillo
-
June 29, 2026
-
0 min