Impact of cerebral small vessel disease burden and systemic clinical phenotypes on short-term neurological outcomes after acute ischemic stroke - Report - MDSpire
Advertisement
Impact of cerebral small vessel disease burden and systemic clinical phenotypes on short-term neurological outcomes after acute ischemic stroke
Clinical Report: Influence of CSVD on Neurological Recovery After AIS
Overview
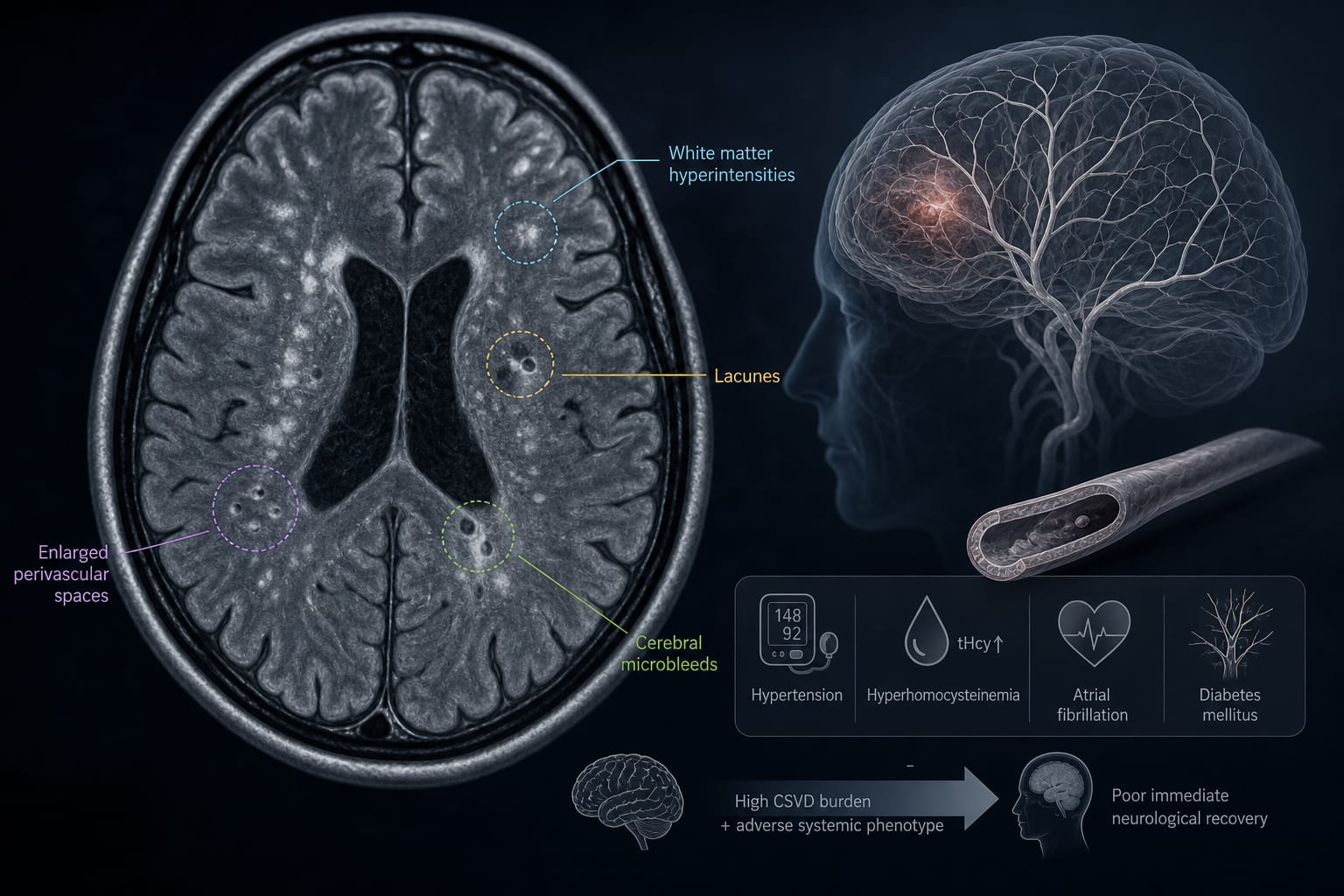
This study investigates the impact of cerebral small vessel disease (CSVD) severity and systemic clinical characteristics on early neurological recovery following acute ischemic stroke (AIS). Findings indicate that higher CSVD burden and specific systemic phenotypes are associated with unfavorable outcomes at discharge.
Background
Cerebral small vessel disease (CSVD) is a significant contributor to acute ischemic stroke (AIS) outcomes, yet its role in early neurological recovery is not fully understood. Understanding the relationship between CSVD and systemic clinical characteristics can help identify patients at risk for poor recovery, which is crucial for optimizing treatment strategies. This study aims to clarify these associations to improve early risk stratification in AIS patients.
Data Highlights
Characteristic
Adjusted Odds Ratio (OR)
95% Confidence Interval (CI)
Total CSVD Burden
1.57
1.13–2.17
Hyperhomocysteinemia
2.76
1.21–6.31
TCM Phlegm-Heat Fu-Excess Phenotype
5.28
1.85–15.04
Lacunar Infarction
Strongest Association
N/A
Key Findings
Higher total CSVD burden is linked to unfavorable neurological outcomes (adjusted OR 1.57).
Hyperhomocysteinemia is associated with increased risk of poor recovery (adjusted OR 2.76).
The TCM-defined Phlegm-Heat Fu-Excess phenotype significantly predicts unfavorable outcomes (adjusted OR 5.28).
Lacunar infarction shows the strongest association with poor discharge NIHSS scores.
White matter hyperintensities and cerebral atrophy correlate with higher NIHSS scores at discharge.
Clinical Implications
Clinicians should consider assessing CSVD burden and systemic clinical phenotypes when evaluating AIS patients for early neurological recovery. Identifying high-risk patients may guide treatment decisions and improve rehabilitation strategies. Further research is needed to validate these findings in larger cohorts.
Conclusion
The study highlights the importance of CSVD and systemic clinical characteristics in predicting early neurological recovery after AIS. These insights may enhance risk stratification and inform clinical management strategies.