Pediatric Auditory Brainstem Implantation: Surgical Approach and Technique
Overview
This report outlines the surgical approach for pediatric auditory brainstem implantation (ABI) using the retrosigmoid craniotomy. It details the anatomical landmarks, device components, and intraoperative techniques to optimize implant placement adjacent to the cochlear nucleus.
Background
The auditory brainstem implant (ABI) was initially developed for patients with profound hearing loss due to NF2-related schwannomatosis and later adapted for pediatric patients with auditory nerve aplasia. The ABI system consists of internal and external components designed to stimulate the cochlear nucleus directly in the brainstem. Precise anatomical knowledge of the cochlear nucleus and surrounding structures is critical for successful implantation. Three commercial ABI systems are currently available, each requiring careful surgical planning and intraoperative monitoring.
Data Highlights
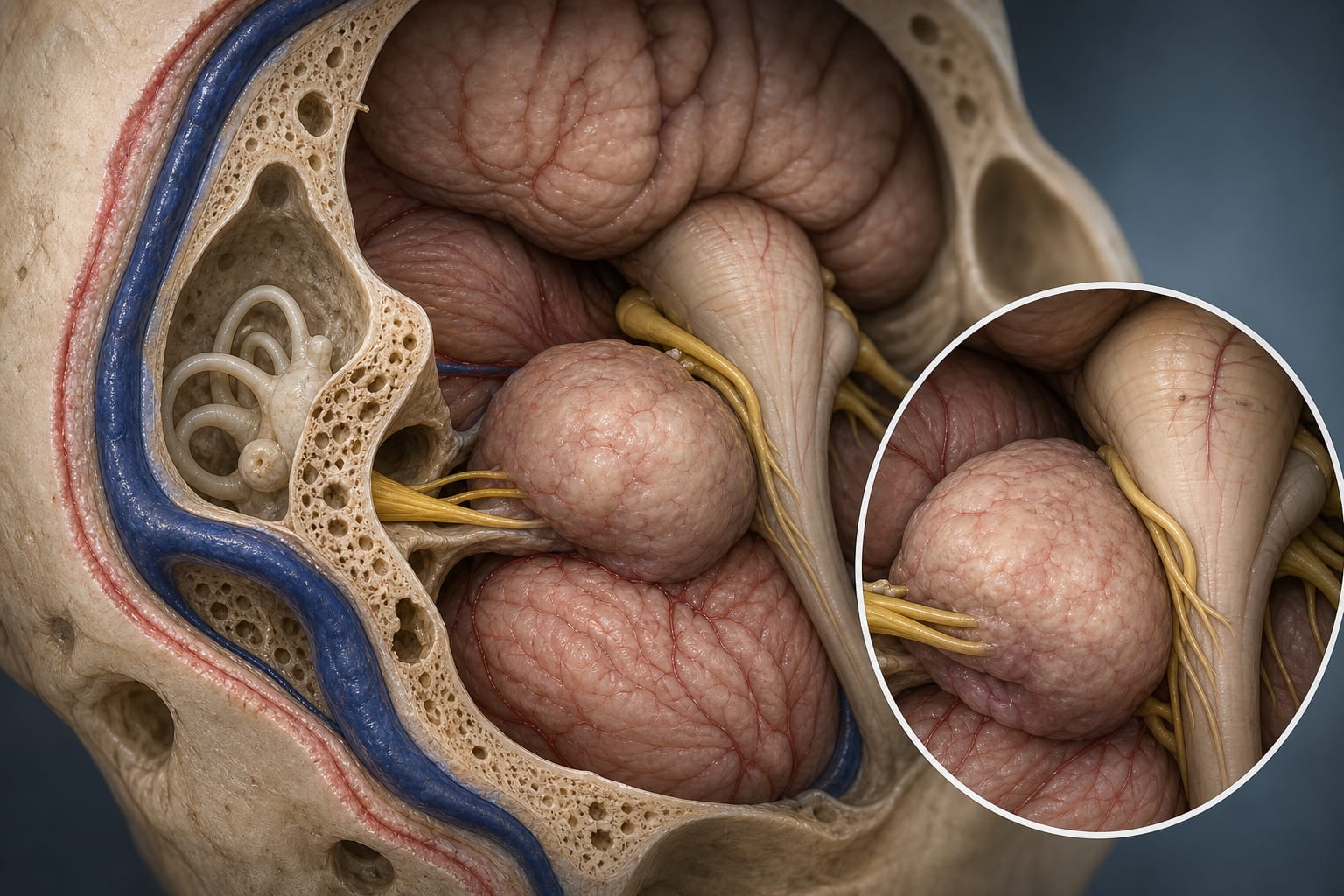
Key intraoperative landmarks include the foramen of Luschka, the 9th cranial nerve, and specific venous structures that guide electrode placement. The retrosigmoid craniotomy approach offers advantages over the translabyrinthine approach by preserving inner ear structures and reducing operative time. The surgical technique involves a 2 × 2.5 cm craniotomy, dural opening in a Y-shape, cerebellar retraction, and precise localization of the lateral recess for electrode placement.
Key Findings
The retrosigmoid craniotomy is preferred for non-NF2 pediatric ABI due to shorter operative time and preservation of inner ear and vestibular function.
Intraoperative landmarks such as the foramen of Luschka, 9th cranial nerve, and choroid plexus are essential for accurate localization of the cochlear nucleus.
Facial nerve monitoring and implant evoked auditory brainstem response (EABR) are used intraoperatively to optimize implant positioning and minimize nerve injury.
A bony well is drilled in the squamous temporal bone to house the receiver-stimulator package, with a channel for the electrode lead to the brainstem.
The ABI electrode paddle, embedded in a Dacron mesh, is trimmed and positioned adjacent to the cochlear nucleus to facilitate effective stimulation.
Clinical Implications
The described retrosigmoid approach allows for effective ABI placement in pediatric patients while preserving critical inner ear structures, potentially improving auditory outcomes. Intraoperative neuromonitoring and anatomical landmarks are vital to minimize complications and optimize electrode positioning. This technique supports individualized surgical planning based on radiological and audiometric assessments.
Conclusion
Pediatric ABI implantation via the retrosigmoid approach is a feasible and effective surgical technique that leverages detailed anatomical knowledge and intraoperative monitoring to enhance outcomes. This method preserves inner ear function and facilitates precise electrode placement adjacent to the cochlear nucleus.
References
Colletti et al. 2001 -- First Pediatric ABI Surgery for Auditory Nerve Aplasia
House Ear Institute 1970s -- Development of Auditory Brainstem Implant
Burnout is easing. Sleep science is getting weird. And dental schools have been winging cadaver training for 50 years. This week's research is full of good news that immediately complicates itself.
The nurse practitioner profession claims the No. 1 spot across three categories in the U.S. News & World Report 2026 Best Jobs rankings for the third consecutive year.