Clinical Report: Comparative Analysis of DLI vs Second Allo-HCT in Relapse
Overview
This study compares therapeutic donor lymphocyte infusion (DLI) and second allogeneic hematopoietic cell transplantation (allo-HCT) in patients with acute leukemia or myelodysplastic syndromes after relapse. No significant difference in overall survival (OS) was observed between the two interventions, highlighting the need for individualized treatment approaches.
Background
Relapse is a leading cause of treatment failure following allogeneic hematopoietic cell transplantation (allo-HCT) in acute leukemia and myelodysplastic syndromes (MDS). Both DLI and second allo-HCT are common post-relapse strategies, yet comparative data are limited. Understanding the efficacy and outcomes of these interventions is crucial for optimizing patient management in this challenging clinical scenario.
Data Highlights
Intervention
Median OS (years)
p-value
DLI
0.92
0.295
Second allo-HCT
0.61
Key Findings
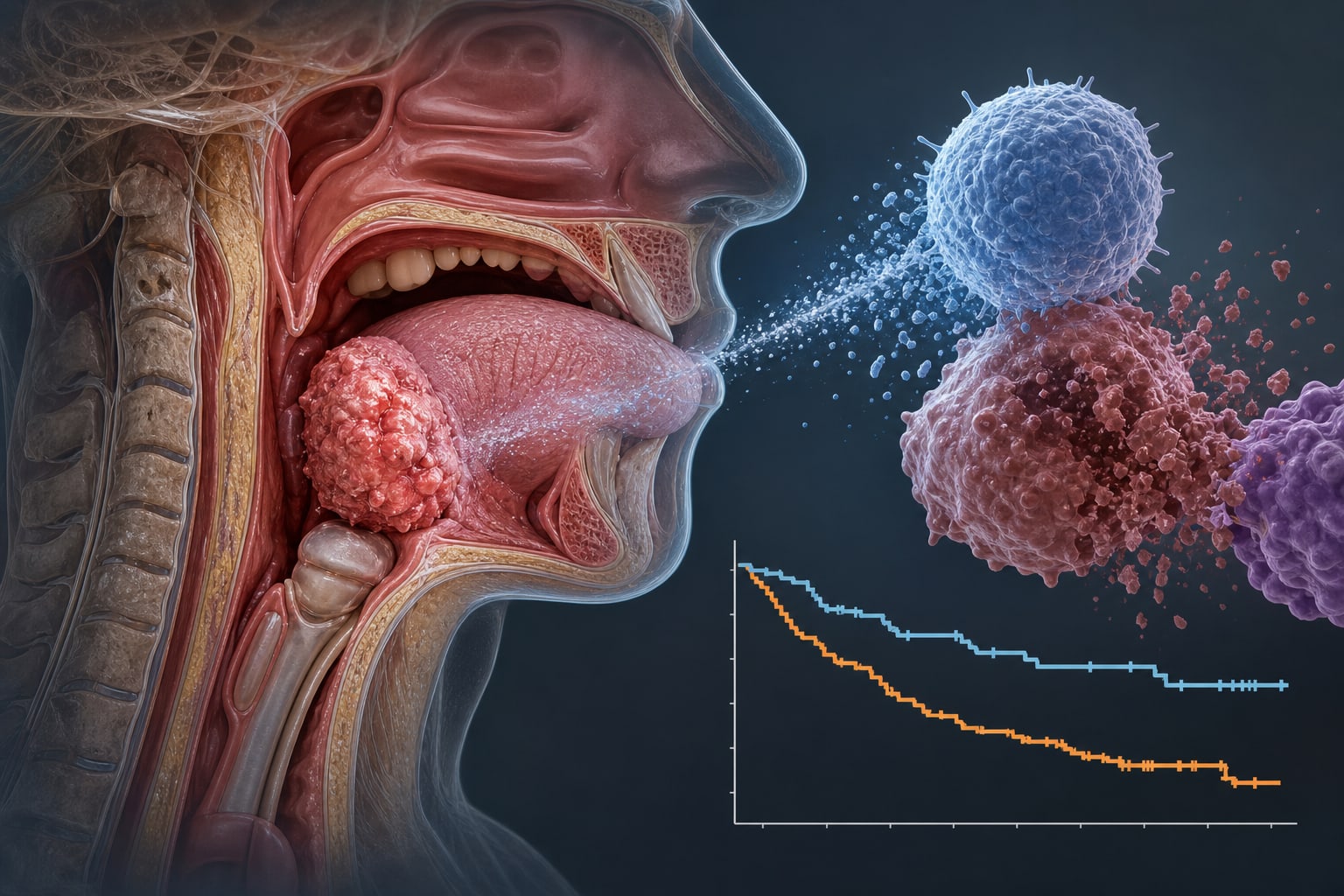
No significant difference in overall survival (OS) between DLI and second allo-HCT (median OS 0.92 vs. 0.61 years, p=0.295).
DLI was associated with higher relapse-related mortality (RRM).
Second allo-HCT showed a trend toward higher non-relapse mortality (NRM).
In a matched cohort of 36 patients, OS remained numerically longer after second allo-HCT without statistical significance.
Individualized treatment approaches are necessary based on patient characteristics and clinical judgment.
Clinical Implications
Clinicians should consider both DLI and second allo-HCT as viable options for patients experiencing relapse after allo-HCT, with treatment decisions tailored to individual patient circumstances. Further multicenter studies are warranted to refine patient selection criteria and optimize outcomes.
Conclusion
The findings indicate that there is no significant survival advantage between DLI and second allo-HCT in relapsed acute leukemia and MDS, underscoring the importance of personalized treatment strategies.