Clinical Report: Forecasting Axillary Lymph Node Metastasis Prior to Surgery
Overview
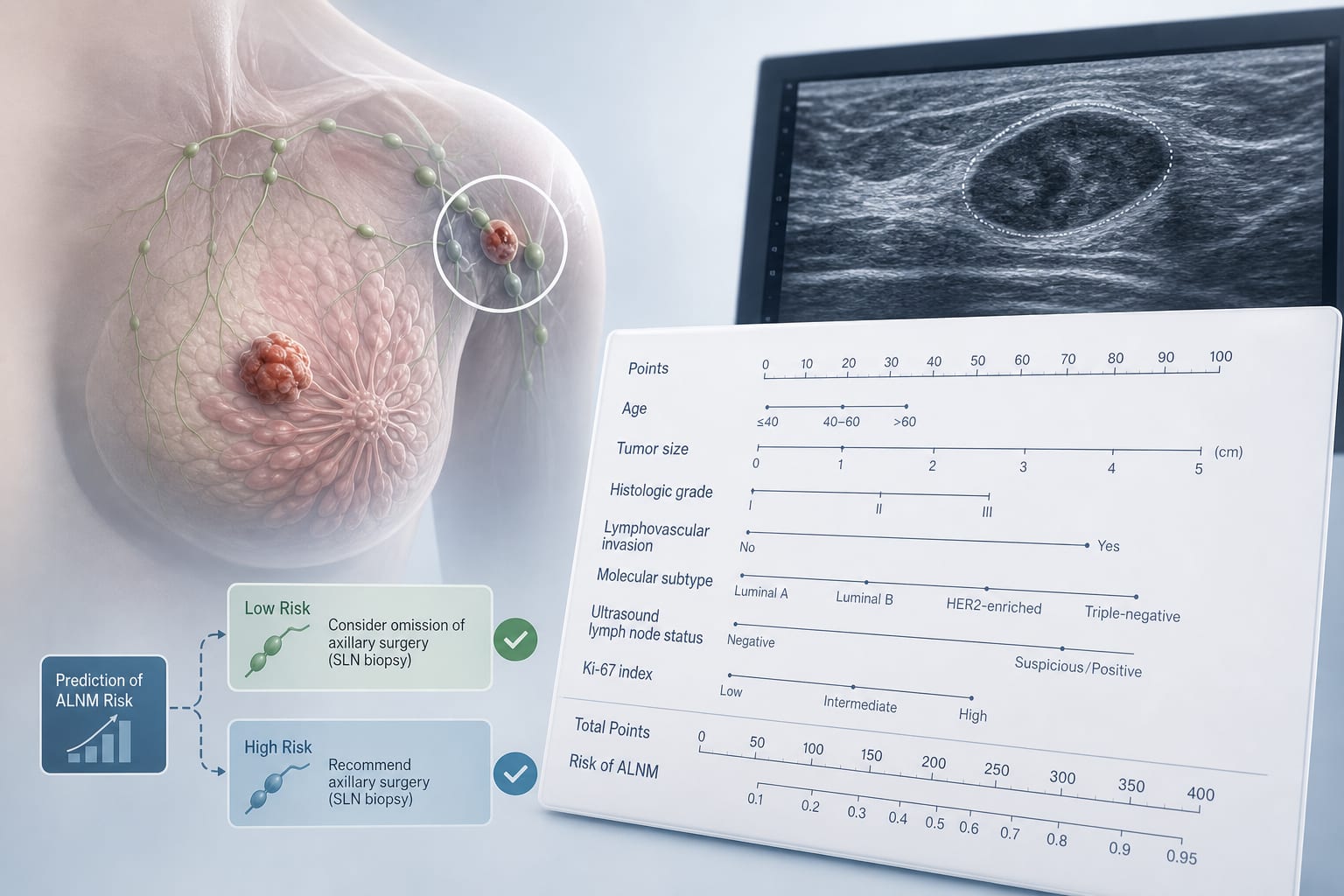
This study evaluates a nomogram for predicting axillary lymph node metastasis (ALNM) in invasive breast cancer (IBC) patients. The model integrates various clinical indicators and demonstrates moderate predictive performance.
Background
Accurate identification of ALNM is crucial in managing invasive breast cancer, as it influences surgical decisions and treatment strategies. Current methods, such as sentinel lymph node biopsy, have limitations, including false-negative rates.
Data Highlights
Group
ALNM Rate
AUC
Training
31.4%
0.741
Validation
27.4%
0.705
Key Findings
ALNM rates were 31.4% in the training group and 27.4% in the validation group.
Independent risk factors for ALNM included tumor size, circumscribe margin, ultrasonic lymph node status, WBC, ER, and BI-RADS.
The nomogram achieved AUCs of 0.741 in the training group and 0.705 in the validation group.
Ultrasonic lymph node status alone had AUCs of 0.620 and 0.627 in the training and validation cohorts, respectively.
Clinical Implications
The nomogram can assist clinicians in preoperative risk stratification for ALNM in IBC patients.
Conclusion
The integration of clinicopathological, ultrasonic, and serological indicators in the nomogram enhances the prediction of ALNM.