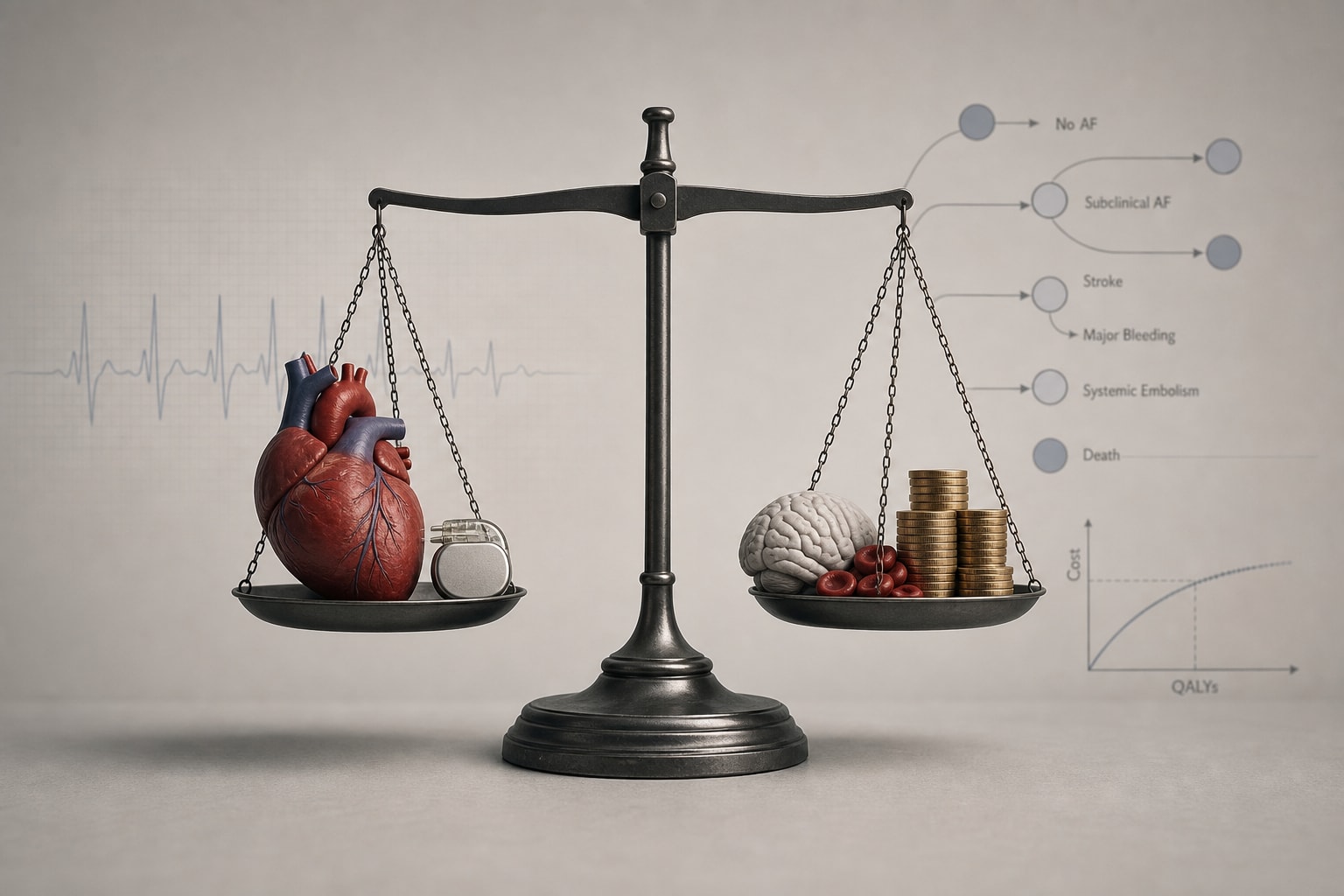
Cost-Effectiveness of Anticoagulation Treatment for Subclinical Device-Detected Atrial Fibrillation
-
By
-
Aleksi K. Winstén
-
Ville Langén
-
K.E. Juhani Airaksinen
-
Konsta Teppo
-
June 8, 2026
-
0 min