Clinical Report: Selection of Dissection Planes in Endoscopic Brow Lifts
Overview
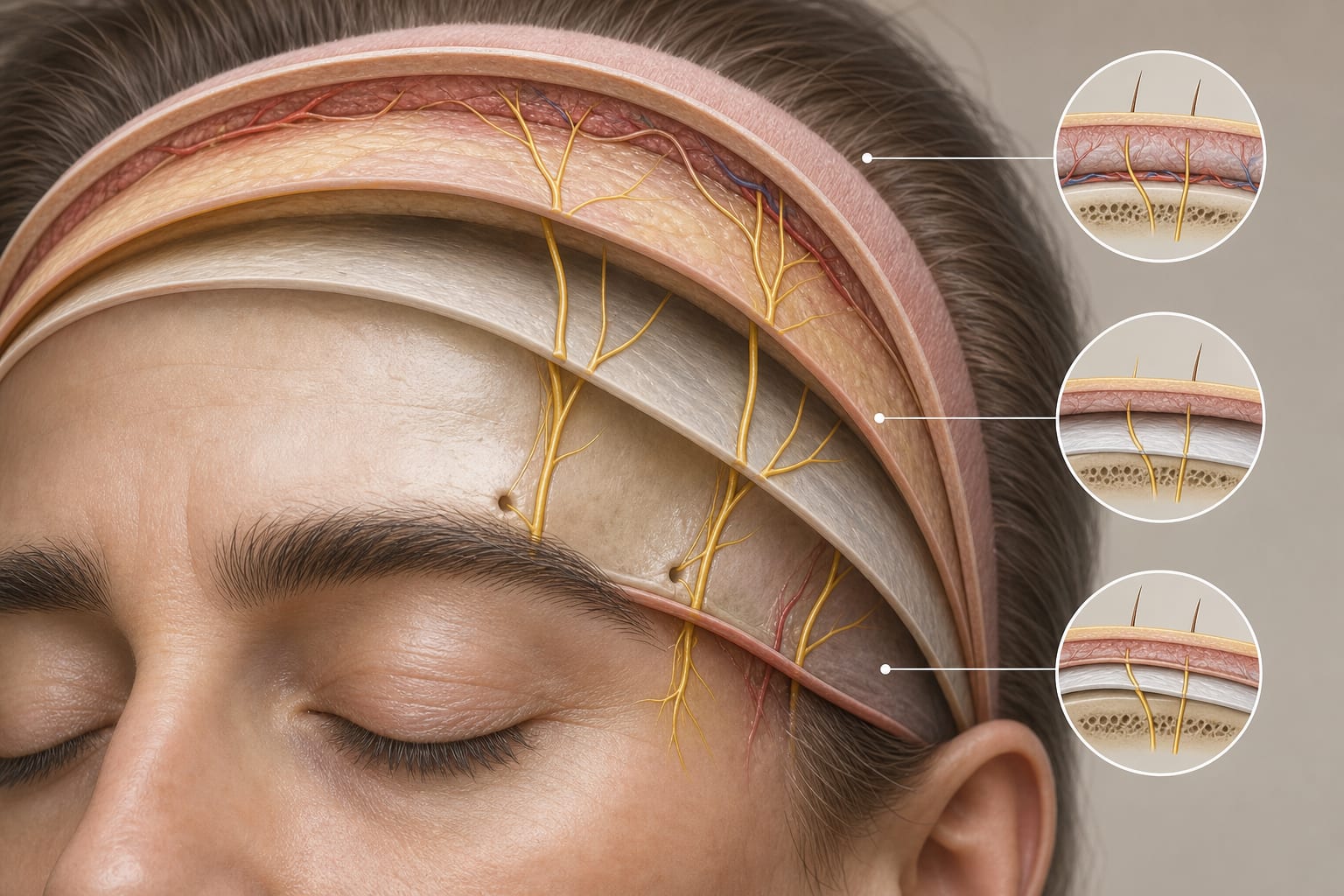
This review compares three principal dissection planes used in endoscopic brow lifts: supraperiosteal, subperiosteal, and combined techniques. It emphasizes the anatomical considerations and risks associated with each approach, particularly concerning the supraorbital nerve.
Background
Endoscopic brow lifts have gained popularity due to their minimally invasive nature, resulting in reduced scarring and shorter recovery times compared to traditional methods. Understanding the anatomical relationships and risks associated with different dissection planes is crucial.
Data Highlights
This review synthesizes anatomical insights and clinical evidence regarding the three dissection approaches without providing specific numerical data.
Key Findings
Three principal dissection planes are used in endoscopic brow lifts: supraperiosteal, subperiosteal, and combined.
Each approach has distinct anatomical relationships and biomechanical lifting mechanisms.
Risk of neurovascular injury, particularly to the deep branch of the supraorbital nerve, varies among the techniques.
Recent studies indicate that supraorbital nerve tension limits brow elevation, necessitating careful consideration of dissection plane selection.
Anatomical variability in the course of the supraorbital nerve complicates surgical standardization.
The combined multiplane approach may balance surgical efficacy with complication avoidance.
Clinical Implications
Surgeons should consider the anatomical considerations and risks associated with each dissection plane when planning endoscopic brow lifts.
Conclusion
The review highlights the importance of anatomical insights in selecting dissection planes for endoscopic brow lifts.