Analysis of Risk Factors for Heart Failure in Patients with Type 2 Diabetes Mellitus and Acute ST-Segment Elevation Myocardial Infarction after Percutaneous Coronary Intervention - Report - MDSpire
Advertisement
Analysis of Risk Factors for Heart Failure in Patients with Type 2 Diabetes Mellitus and Acute ST-Segment Elevation Myocardial Infarction after Percutaneous Coronary Intervention
Clinical Report: Independent Risk Factors for Heart Failure in T2DM Patients
Overview
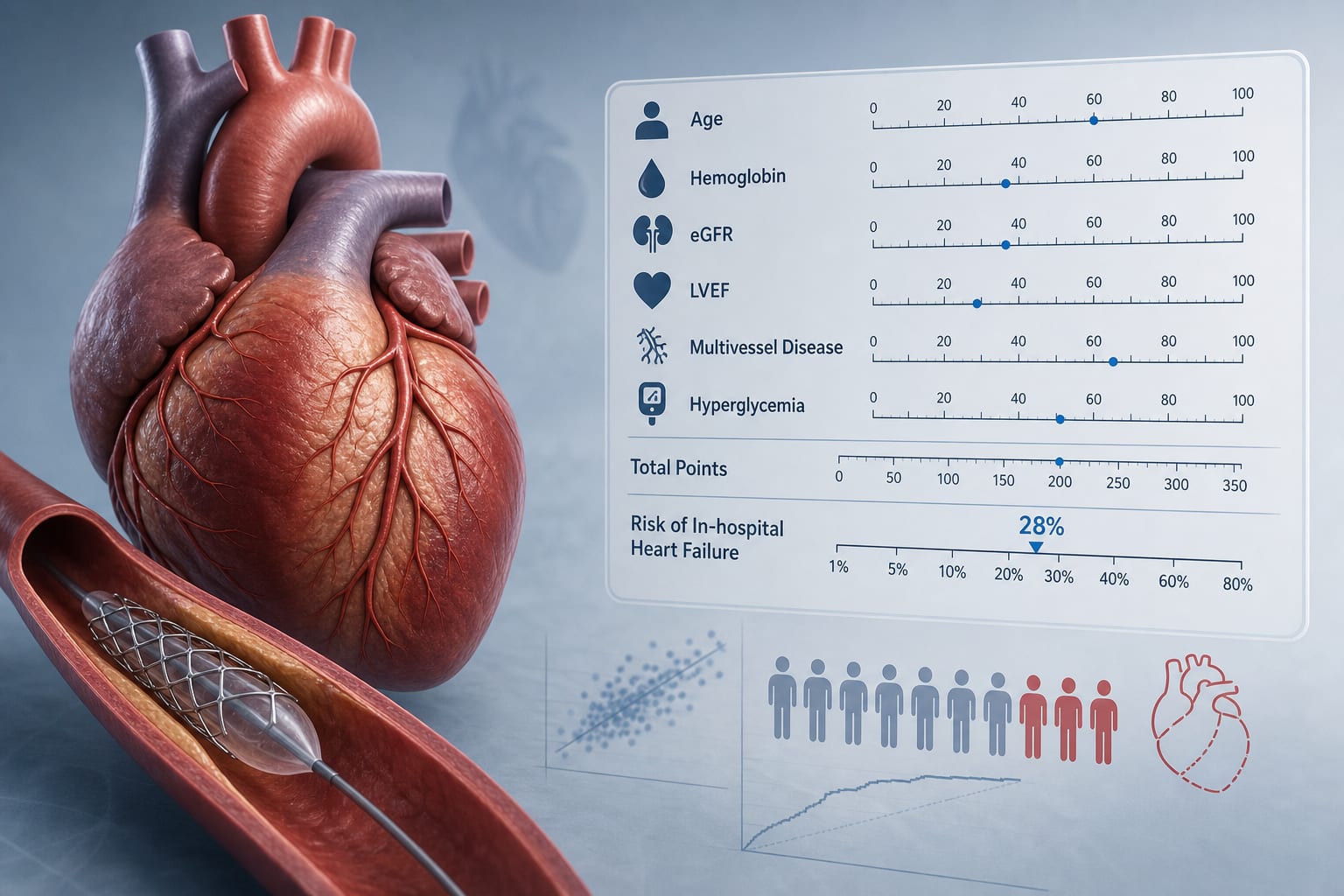
This study identifies seven independent risk factors for in-hospital heart failure (HF) in patients with type 2 diabetes mellitus (T2DM) and acute ST-segment elevation myocardial infarction (STEMI) post-percutaneous coronary intervention (PCI). A nomogram prediction model was developed, demonstrating strong predictive capability and calibration.
Background
Heart failure is a significant complication following myocardial infarction, particularly in patients with T2DM, who are at increased risk due to underlying pathophysiological factors. Identifying risk factors for HF in this population can enhance clinical decision-making and improve patient outcomes. This study aims to provide a predictive tool to identify high-risk patients early in their hospital course.
Seven independent risk factors for in-hospital HF were identified: prior myocardial infarction, smoking history, diminished left ventricular ejection fraction, heightened white blood cell count, reduced hemoglobin level, increased platelet count, and atrial fibrillation.
The nomogram model showed an area under the curve (AUC) of 0.845, indicating strong predictive capability.
Calibration of the nomogram was confirmed with a Hosmer-Lemeshow goodness-of-fit test (P=0.712).
Sensitivity analysis demonstrated the model's stability with no significant multicollinearity (all VIF <1.5).
External validation of the nomogram is necessary before clinical application.
Clinical Implications
Healthcare professionals should consider these identified risk factors when assessing patients with T2DM and STEMI for potential heart failure. The nomogram can serve as a preliminary tool for early identification of high-risk patients, guiding clinical interventions and monitoring strategies.
Conclusion
The study provides valuable insights into the risk factors for heart failure in T2DM patients post-PCI, along with a promising predictive model. Further external validation is essential to establish its clinical utility.