Preoperative CT markers and poor discharge functional status after burr-hole drainage for chronic subdural hematoma: a retrospective cohort study - Scorecard - MDSpire
Advertisement
Preoperative CT markers and poor discharge functional status after burr-hole drainage for chronic subdural hematoma: a retrospective cohort study
Clinical Scorecard: Preoperative CT Indicators and Adverse Functional Outcomes Following Burr-Hole Drainage for Chronic Subdural Hematoma: A Retrospective Analysis
At a Glance
Category
Detail
Condition
Chronic Subdural Hematoma (CSDH)
Key Mechanisms
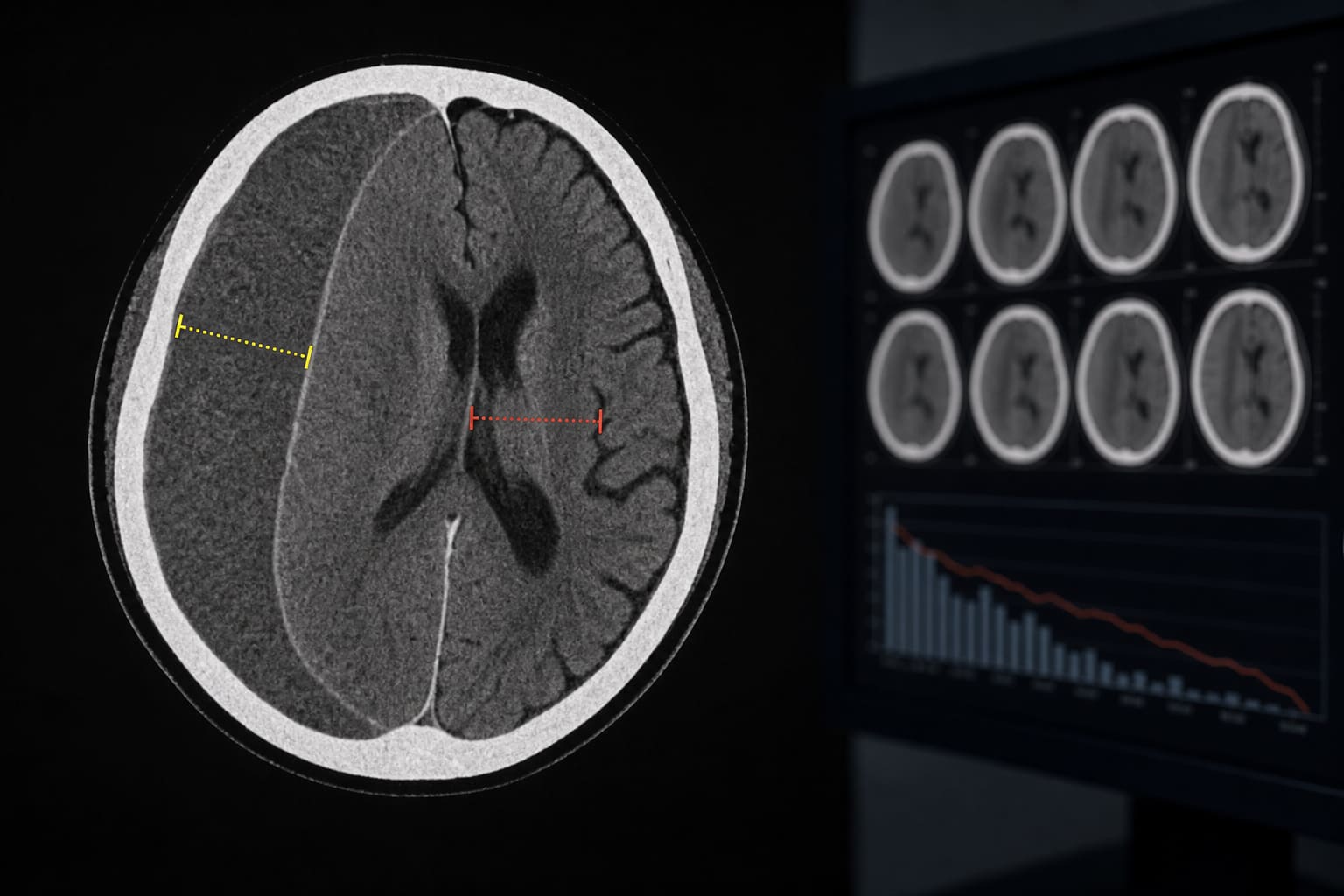
Preoperative CT markers including hematoma thickness and midline shift.
Target Population
Adult patients undergoing burr-hole drainage for CSDH.
Care Setting
Single-center neurosurgery department.
Key Highlights
25.4% of patients had poor discharge functional status (mRS ≥3).
Midline shift, pre-hospital mRS, and age were independently associated with poor outcomes.
Hematoma thickness showed a numerical association but did not meet statistical significance.
Study utilized multivariable logistic regression and restricted cubic spline analysis.
Findings are exploratory and require external validation.
Guideline-Based Recommendations
Diagnosis
Evaluate preoperative CT markers such as hematoma thickness and midline shift.
Management
Consider age and pre-existing functional status in preoperative risk stratification.
Monitoring & Follow-up
Adjust postoperative monitoring intensity based on preoperative indicators.
Risks
Patients may experience persistent functional disability post-surgery.
Patient & Prescribing Data
260 consecutive adult patients with CSDH.
Burr-hole drainage is the most common surgical treatment.
Clinical Best Practices
Incorporate preoperative CT findings into patient counseling.
Utilize established clinical factors alongside radiological indicators for outcome prediction.