Modified surgical technique for recurrent organized chronic subdural hematoma: a preliminary retrospective case series
-
By
-
Sheng Li
-
Guangzhao Li
-
Yulong Wang
-
Jianwen Wang
-
Guanhang Shu
-
Xiaowang Niu
-
Xiang Li
-
June 23, 2026
-
Clinical Scorecard: Innovative Surgical Approach for Recurrent Organized Chronic Subdural Hematoma: An Initial Retrospective Case Analysis
At a Glance
| Category | Detail |
|---|
| Condition | Recurrent Organized Chronic Subdural Hematoma |
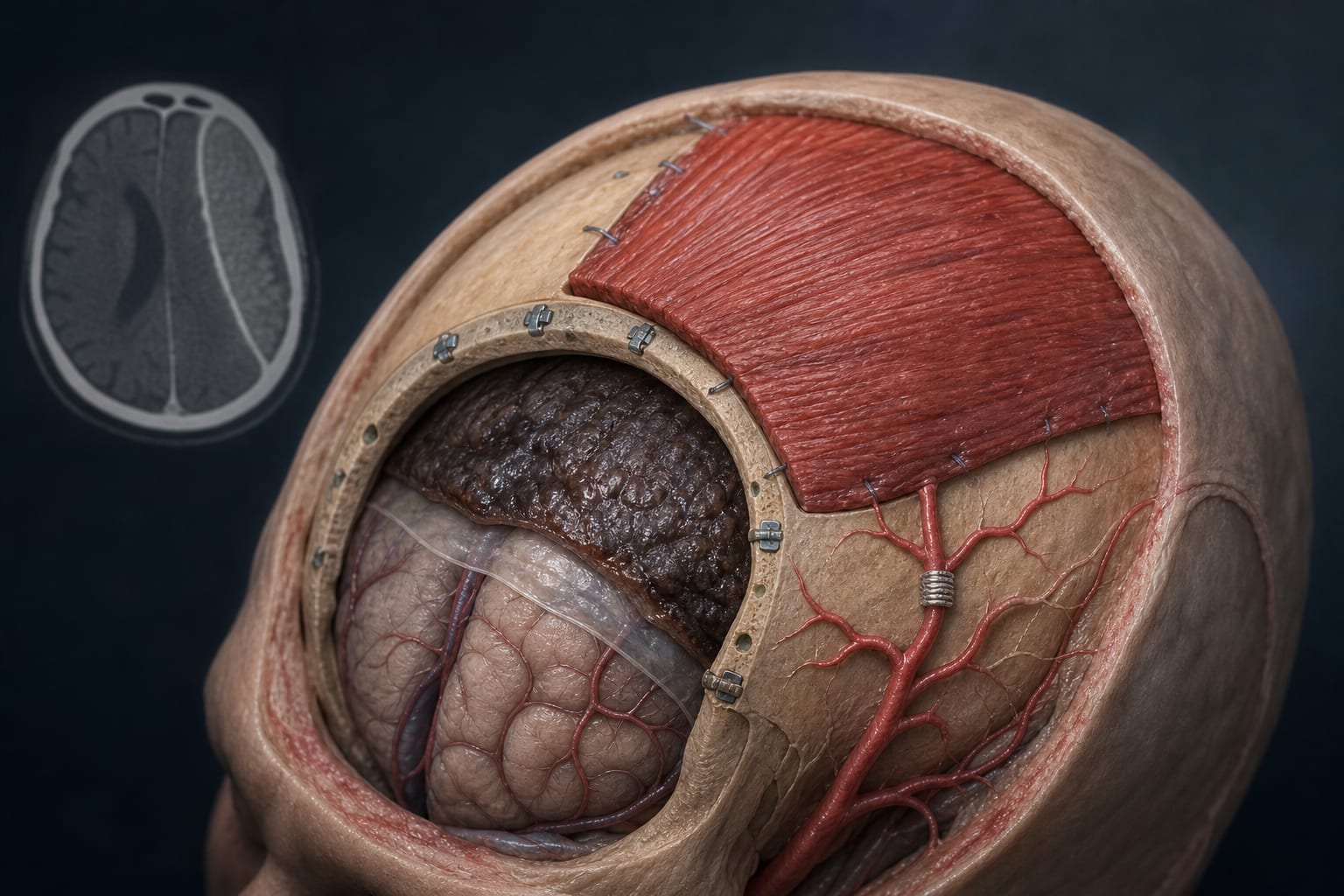
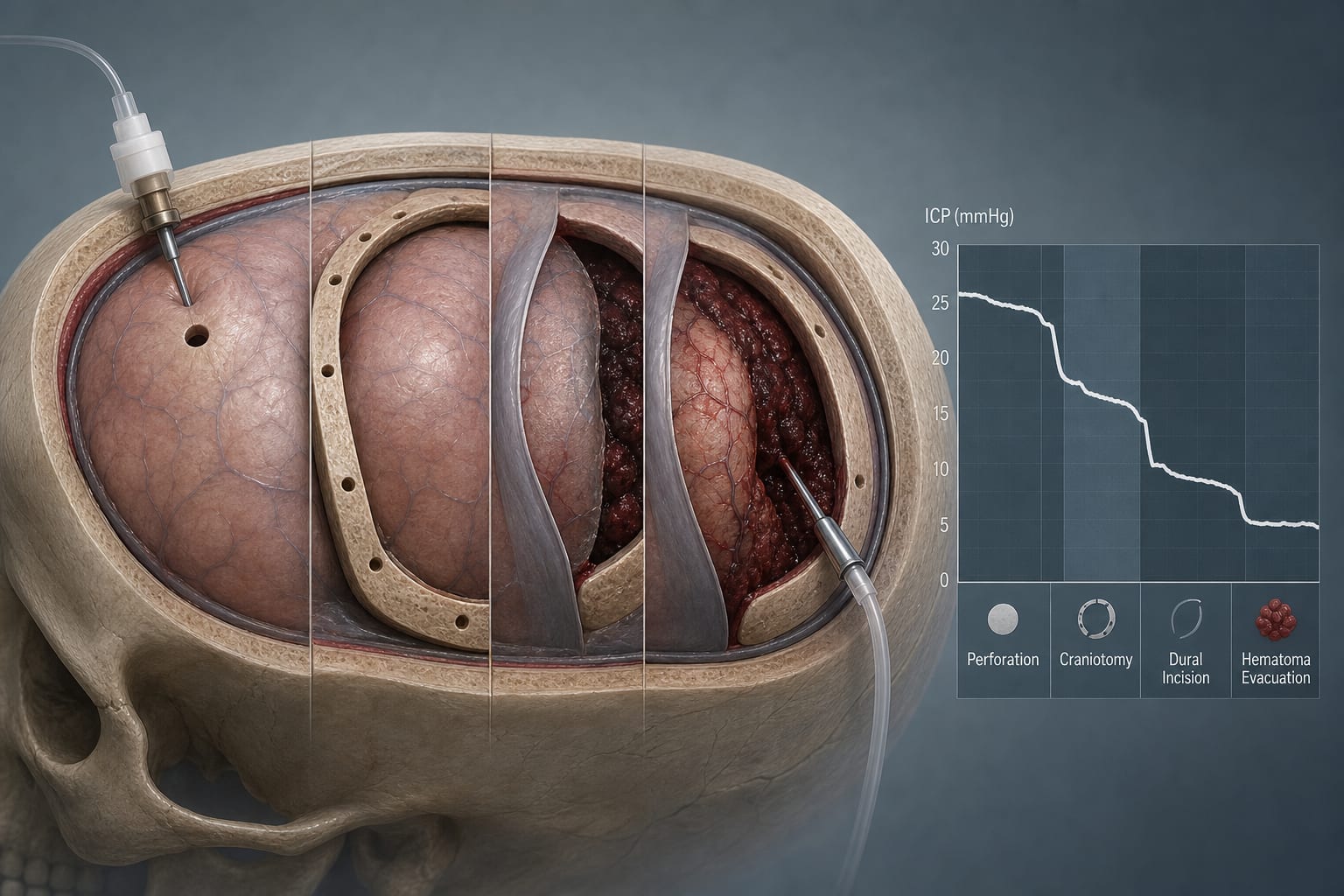
| Key Mechanisms | Craniotomy for hematoma evacuation combined with middle meningeal artery occlusion and temporalis muscle grafting. |
| Target Population | Patients aged 63-82 years with recurrent organized CSDH. |
| Care Setting | Surgical treatment in a hospital setting. |
Key Highlights
- Complete hematoma evacuation achieved in all patients.
- Improvement in neurological function postoperatively as measured by GCS, mRS, Markwalder grade, and GOS scores.
- Postoperative complications occurred in 29.41% of patients but resolved with conservative management.
- No recurrence observed within 90 days post-surgery.
- Study involved a highly selected cohort of 17 patients.
Guideline-Based Recommendations
Diagnosis
- Diagnosis of organized CSDH based on clinical history, cranial CT/MRI findings, and intraoperative observation.
Management
- Modified craniotomy technique for hematoma evacuation is recommended for recurrent organized CSDH.
Monitoring & Follow-up
- Monitor for postoperative complications and recurrence during follow-up.
Risks
- Potential complications include subdural effusion, cerebrospinal fluid leak, secondary intracranial hemorrhage, and epilepsy.
Patient & Prescribing Data
17 patients with recurrent organized CSDH, previously treated with burr-hole drainage.
Modified surgical approach shows preliminary safety and feasibility.
Clinical Best Practices
- Consider craniotomy for organized hematomas that cannot be effectively treated with burr-hole drainage.
- Evaluate neurological function using standardized scales postoperatively.
Related Resources & Content