Prognostic model for three-year postoperative local recurrence in cutaneous squamous cell carcinoma: a Chinese multicenter cohort study - Scorecard - MDSpire
Advertisement
Prognostic model for three-year postoperative local recurrence in cutaneous squamous cell carcinoma: a Chinese multicenter cohort study
Clinical Scorecard: Development of a Prognostic Nomogram for Three-Year Local Recurrence Risk in Cutaneous Squamous Cell Carcinoma: Findings from a Multicenter Study in China
At a Glance
Category
Detail
Condition
Cutaneous Squamous Cell Carcinoma (cSCC)
Key Mechanisms
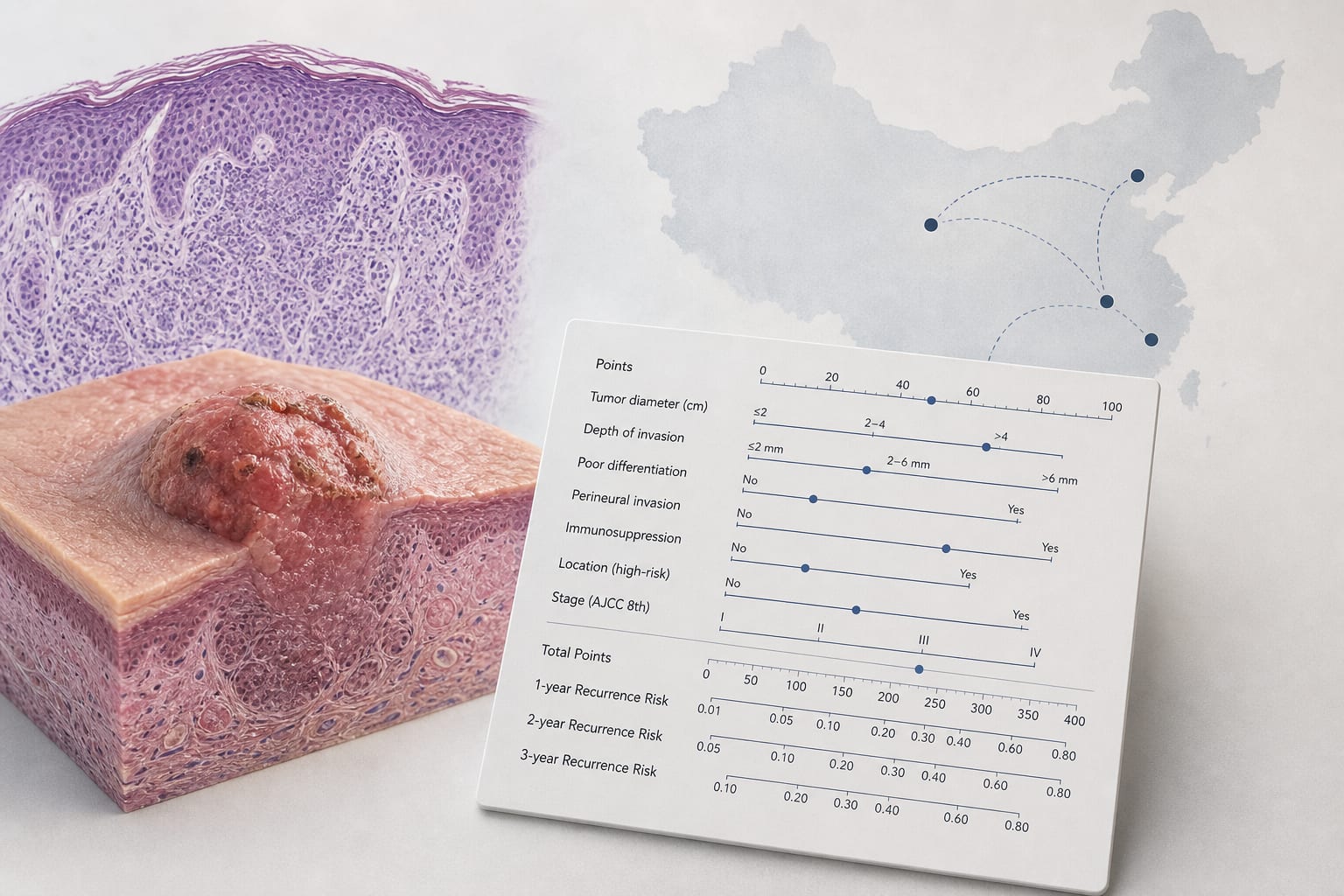
Independent predictors of postoperative local recurrence include age, tumor size, tumor thickness, histologic differentiation, regional stage, and AJCC stage.
Target Population
Patients with biopsy-confirmed cSCC who underwent surgical treatment in China.
Care Setting
Multicenter study across four hospitals in China.
Key Highlights
90% of local recurrence events occur within 3 years post-surgery.
Nomogram developed to predict individualized 1-, 2-, and 3-year recurrence probabilities.
Patients stratified into low-, intermediate-, and high-risk groups based on nomogram scores.
Multivariable analysis identified six independent predictors of recurrence.
Model demonstrated good discrimination with AUC values from 0.759 to 0.869.
Guideline-Based Recommendations
Diagnosis
Biopsy-confirmed cSCC with negative surgical margins.
Management
Surgical treatment is the primary management for cSCC.
Monitoring & Follow-up
Postoperative risk stratification for surveillance strategies based on nomogram scores.
Risks
Increased risk of local recurrence associated with specific clinicopathological features.
Patient & Prescribing Data
603 patients with cSCC from four Chinese centers.
Surgical excision is the most common treatment; high-risk features may necessitate closer monitoring.
Clinical Best Practices
Utilize the nomogram for individualized prognostic assessment.
Incorporate risk stratification into follow-up management.
The clinical-stage cancer biotech raised $670 million in an upsized Nasdaq debut, with a further $75 million expected from a concurrent Regeneron private placement