Practice variations in indication, timing and outcome of Multiple Myeloma patients undergoing surgery for vertebral lesions – results from the European M2Spine study group - Scorecard - MDSpire
Advertisement
Practice variations in indication, timing and outcome of Multiple Myeloma patients undergoing surgery for vertebral lesions – results from the European M2Spine study group
Clinical Scorecard: Variability in Surgical Indications, Timing, and Outcomes for Vertebral Lesions in Multiple Myeloma Patients: Findings from the European M2Spine Study Group
At a Glance
Category
Detail
Condition
Multiple Myeloma with vertebral column lesions
Key Mechanisms
Plasma cell malignancy causing bone lesions leading to fractures, pain, neurological deficits; bone fragility and immunocompromise complicate surgical decisions
Target Population
Adult patients (≥18 years) with symptomatic vertebral lesions due to Multiple Myeloma
Care Setting
Tertiary academic spine centers with interdisciplinary teams including spine surgery, hematology, oncology, and radio-oncology
Key Highlights
80% of MM patients develop bone complications; 50% involve vertebral lesions causing fractures, pain, and neurological risks
Non-surgical management predominates due to MM sensitivity to radio- and chemotherapy and high surgical infection risk
Surgical intervention considered when non-surgical treatment fails, especially for spinal instability or neurological deficits
Guideline-Based Recommendations
Diagnosis
Use ICD-10 codes C90 (Multiple Myeloma) and C79 (vertebral column lesion) for patient identification
Assess vertebral lesions with CT and MRI imaging
Evaluate spinal stability using Spinal Instability Neoplastic Score (SINS)
Assess neurological and ambulatory status with modified McCormick Scale
Management
Predominantly non-surgical treatment including radio- and chemotherapy for vertebral lesions
Minimally invasive cement augmentation for persistent vertebral pain to reduce pain and improve independence
Surgical approaches (posterior instrumentation, fusion, decompression) reserved for spinal instability, neurological deficits, or failure of conservative treatment
Monitoring & Follow-up
Regular follow-up with clinical and imaging assessments to monitor lesion progression and neurological status
Use ECOG, Karnofsky (KPS), and ASA scores to assess patient functional status during treatment
Monitor for complications post-surgery and neurological outcomes
Risks
High risk of surgical site infections due to immunocompromised status
Potential for delayed surgical intervention impacting neurological outcomes
Cement augmentation does not restore spinal stability or prevent deformities
Patient & Prescribing Data
Adult MM patients with symptomatic vertebral lesions treated between 2005 and 2023 at European tertiary centers
Interdisciplinary treatment decisions vary; lack of standardized surgical guidelines leads to variability in timing and indications for surgery
Clinical Best Practices
Employ interdisciplinary teams for comprehensive management of MM vertebral lesions
Use standardized scoring systems (SINS, Bilsky, McCormick) to guide treatment decisions
Prioritize non-surgical treatments initially due to MM radiosensitivity and infection risks
Consider minimally invasive cement augmentation for pain relief when conservative treatment fails
Reserve surgical intervention for spinal instability, neurological deficits, or refractory symptoms
Collect and analyze multicenter data to inform future evidence-based guidelines
by Vanessa Hubertus, Lennart Viezens, Martin Stangenberg, Anton M. Früh, Hanno S. Meyer, Raimunde Liang, Andreas Kramer, Christoph Orban, Johannes Kerschbaumer, Beate Kunze, Stefano Telera, Hannah Miller, Christian J. Entenmann, Emily J. von Bronewski, Charlotte Buhre, Leon-Gordian Leonhardt, Wolfgang Willenbacher, Irma Kvitsaridze, Dominik Laue, Matthias Pumberger, Theresa Keller, Güliz Acker, Jan Krönke, Igor-Wolfgang Blau, Ulrich Keller, Florian Ringel, Claudius Thomé, Bernhard Meyer, Peter Vajkoczy, Marc Dreimann, Julia Sophie Onken
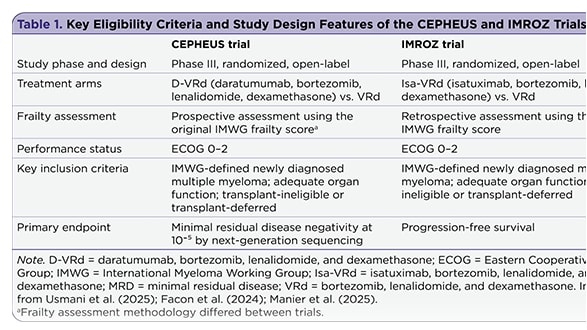
The management of newly diagnosed transplant-ineligible multiple myeloma remains challenging, in part due to the complexity of treatment decisions for frail patients. Recent subgroup analyses provide insight into whether quadruplet therapy may offer advantages over triplet therapy in this population.