Clinical Scorecard: Cellular and Stromal Changes Contributing to Heart Damage from Radiation: Insights Gained Through Single-Cell Transcriptomic Analysis
At a Glance
Category
Detail
Condition
Radiation-induced heart injury (RIHI)
Key Mechanisms
Stromal-immune cascade involving endothelial cell and fibroblast immunogenic reprogramming.
Target Population
Patients undergoing thoracic radiotherapy for lung, breast, and mediastinal malignancies.
Care Setting
Oncology and cardiology settings focusing on late complications of thoracic radiotherapy.
Key Highlights
RIHI incidence rates range from 15% to over 30% based on tumor type and radiation dose.
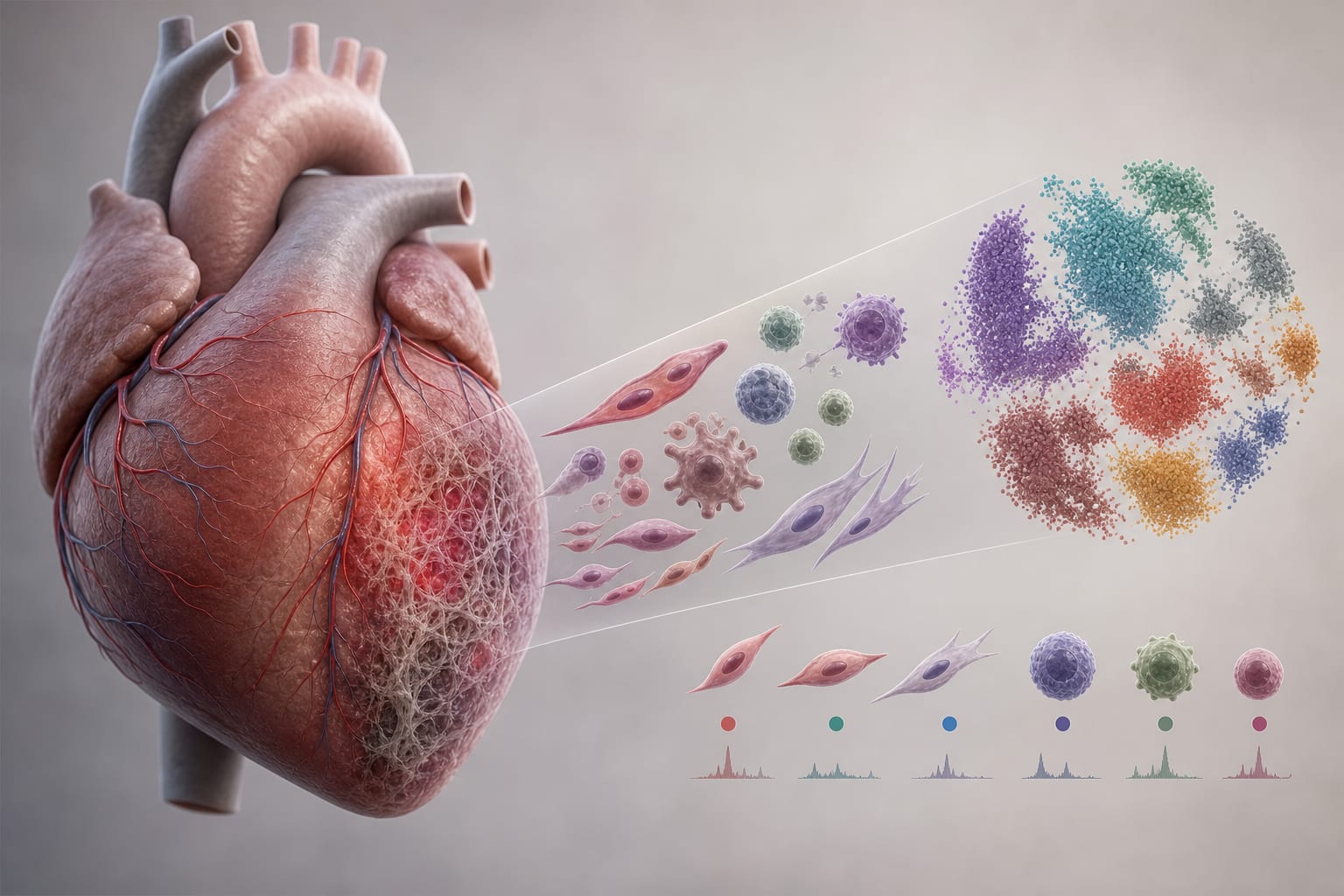
Endothelial cells and fibroblasts undergo significant changes post-irradiation, including MHC-II upregulation.
Myeloid and lymphoid activation leads to a pro-inflammatory cardiac microenvironment.
Single-cell RNA sequencing provides insights into cellular heterogeneity and immune activation in RIHI.
Non-hematopoietic antigen presentation is identified as a potential therapeutic target.
Guideline-Based Recommendations
Diagnosis
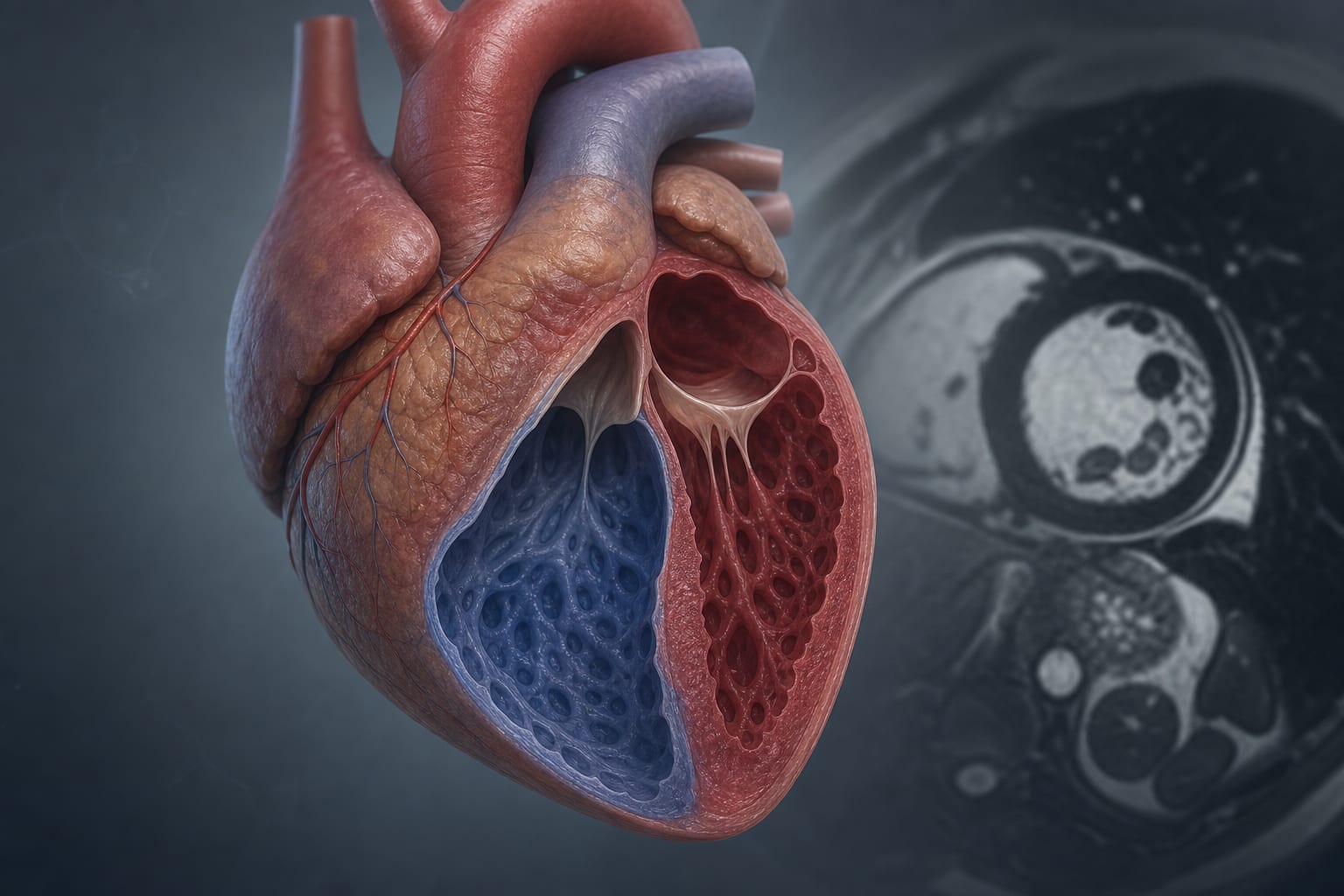
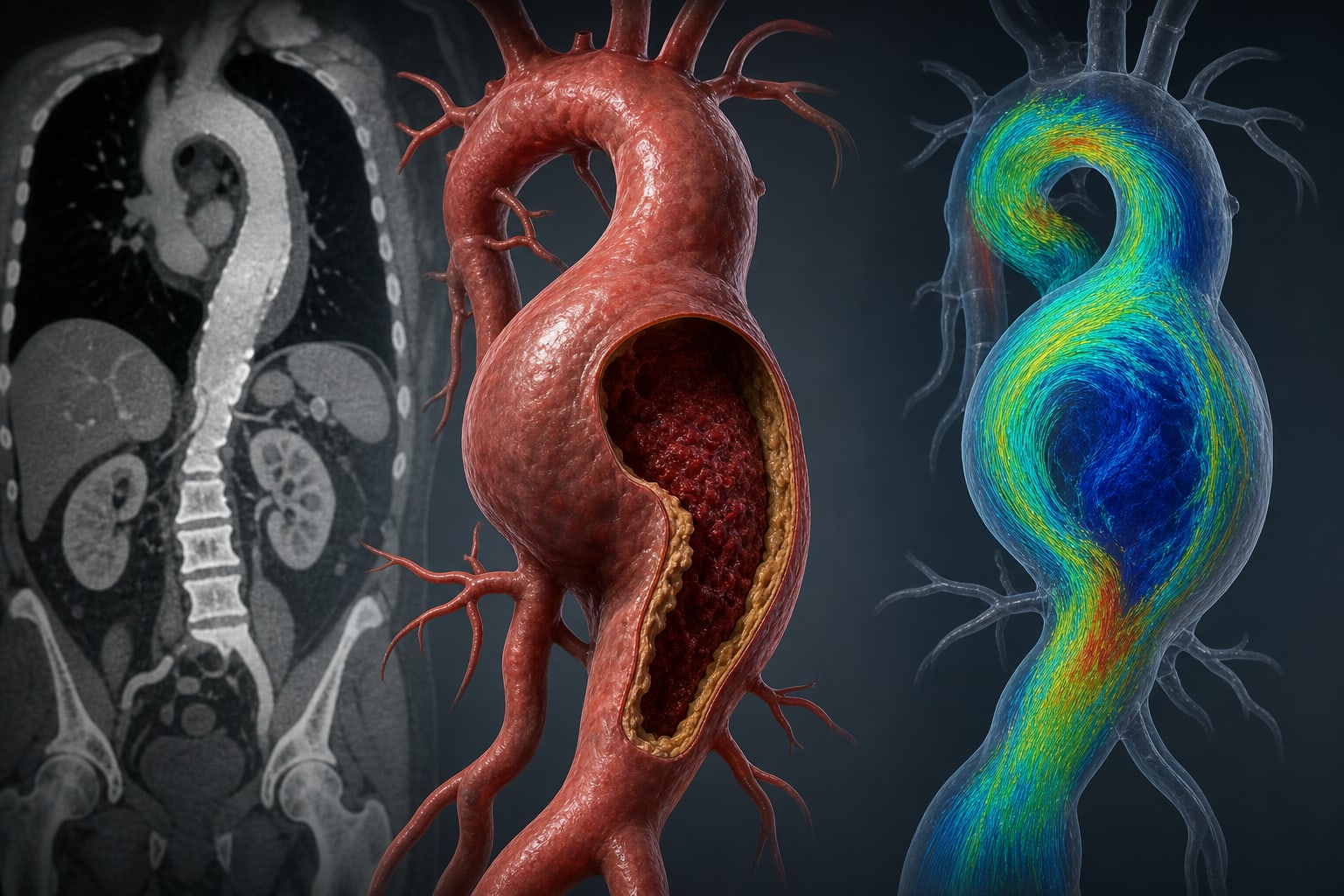
Utilize imaging and histological assessment to evaluate cardiac injury post-radiotherapy.
Management
Consider immunotherapy approaches in conjunction with thoracic radiotherapy.
Monitoring & Follow-up
Regular cardiovascular assessments for patients receiving thoracic radiotherapy.
Risks
Increased cardiovascular morbidity and mortality associated with RIHI.
Patient & Prescribing Data
Patients with lung, breast, and mediastinal cancers undergoing thoracic radiotherapy.
Combination of radiation therapy with immune checkpoint inhibitors may enhance therapeutic outcomes.
Clinical Best Practices
Implement strategies to mitigate RIHI in patients receiving thoracic radiotherapy.
Monitor for signs of cardiac inflammation and dysfunction in at-risk populations.