Clinical Scorecard: Outcomes of COVID-19 in Pediatric Patients with Adrenal Insufficiency: Insights from National Data
At a Glance
Category
Detail
Condition
Adrenal insufficiency (AI) in pediatric patients
Key Mechanisms
Insufficient cortisol production leading to vulnerability to infections and risk of adrenal crisis during infections
Target Population
Children with primary or secondary adrenal insufficiency
Care Setting
Multicenter pediatric endocrinology and infectious disease clinical settings
Key Highlights
Prevalence of COVID-19 in children with AI (12.9%) was not increased compared to the general pediatric population.
Severity of COVID-19 in AI patients was similar to controls, with no increased risk of severe or critical illness.
Adrenal crisis occurred in only 3.4% of AI patients during severe COVID-19; all patients fully recovered with no COVID-related deaths.
Guideline-Based Recommendations
Diagnosis
Diagnose AI based on low basal or stimulated cortisol levels with corresponding ACTH levels (elevated in PAI, low/normal in SAI).
Exclude tertiary AI related to exogenous steroid use.
Exclude patients with adjunctive risk factors such as severe obesity, heart or pulmonary disease, hypertension, malignancy, or immunodeficiency.
Management
Continue glucocorticoid replacement therapy (primarily hydrocortisone) during COVID-19 infection.
Monitor for adrenal crisis during severe infections and manage promptly.
Hospitalization rates for AI patients with COVID-19 are similar to controls; manage according to severity.
Monitoring & Follow-up
Monitor clinical severity of COVID-19 symptoms ranging from asymptomatic to critical.
Watch for development of pneumonia or multisystem inflammatory syndrome (MIS-C).
Observe for signs of adrenal crisis during infection.
Risks
AI does not increase susceptibility to SARS-CoV-2 infection or risk of severe COVID-19 in children.
Adrenal crisis is a potential complication during severe COVID-19 but is infrequent.
No increased mortality risk from COVID-19 in pediatric AI patients was observed.
Patient & Prescribing Data
Pediatric patients with primary or secondary adrenal insufficiency infected with SARS-CoV-2
Glucocorticoid replacement therapy with hydrocortisone remains standard; no evidence of increased COVID-19 severity or hospitalization necessitating treatment modification.
Clinical Best Practices
Exclude patients with additional comorbidities that increase COVID-19 severity risk when assessing AI impact.
Maintain standard glucocorticoid replacement therapy during COVID-19 infection.
Promptly identify and treat adrenal crisis during severe infections.
Use case-control comparisons to evaluate infection prevalence and severity in AI populations.
Educate families on recognizing symptoms of adrenal crisis and COVID-19 severity.
by Donatella Capalbo, Cristina Moracas, Laura Guazzarotti, Federico Baronio, Marianna Rita Stancampiano, Rita Ortolano, Mariella Valenzise, Carla Bizzarri, Giuseppa Patti, Silvia Longhi, Claudia Giavoli, Chiara Guzzetti, Silvia Zoletto, Crescenza Lattanzio, Paolo Cavarzere, Maria Elisabeth Street, Maria Felicia Faienza, Anna Grandone, Marco Cappa, Malgorzata Gabriela Wasniewska, Gianni Russo, Mohamad Maghnie, Mariacarolina Salerno, On behalf of the Study Group for Adrenal Diseases of the Italian Society for Pediatric Endocrinology and Diabetes
This quality improvement project found that using a distress screening tool for head and neck cancer patients who were 2 or more years post-treatment led to an increased number of referrals for psychosocial needs.
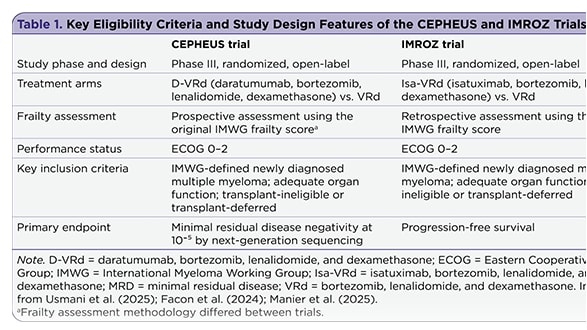
The management of newly diagnosed transplant-ineligible multiple myeloma remains challenging, in part due to the complexity of treatment decisions for frail patients. Recent subgroup analyses provide insight into whether quadruplet therapy may offer advantages over triplet therapy in this population.