Epstein-Barr virus reactivation triggers selective IL-6/IL-10 axis inflammation and CD3+CD8+ T-cell activation leading to severe leukopenia, hyperinflammatory shock, and myocardial injury: a case report - Scorecard - MDSpire
Advertisement
Epstein-Barr virus reactivation triggers selective IL-6/IL-10 axis inflammation and CD3+CD8+ T-cell activation leading to severe leukopenia, hyperinflammatory shock, and myocardial injury: a case report
Clinical Scorecard: Reactivation of Epstein-Barr Virus Induces Targeted IL-6/IL-10 Axis Inflammation and Activation of CD3+CD8+ T Cells Resulting in Severe Leukopenia, Hyperinflammatory Shock, and Cardiac Injury: A Case Study
At a Glance
Category
Detail
Condition
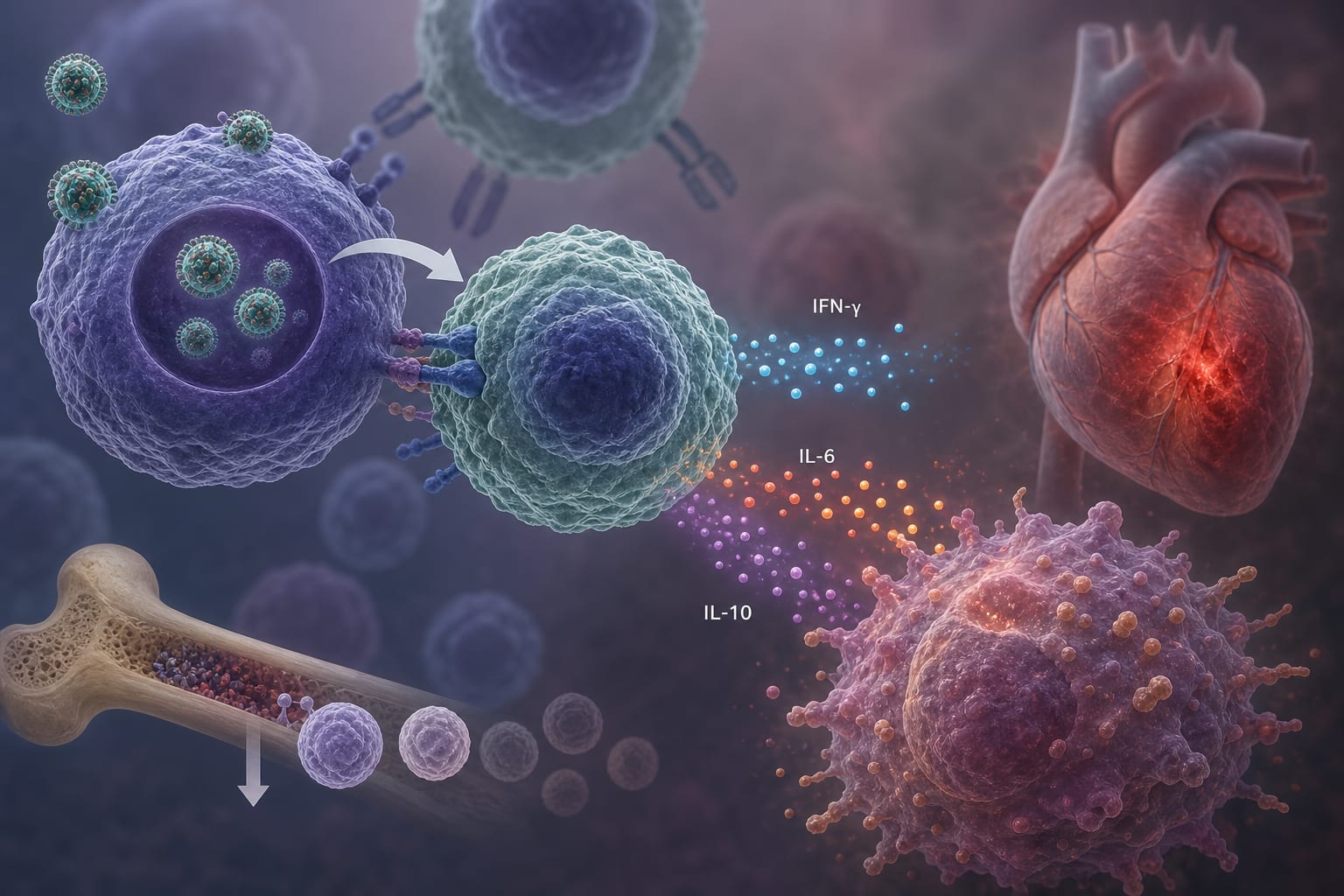
Epstein-Barr Virus Reactivation
Key Mechanisms
IL-6/IL-10 axis inflammation and CD3+CD8+ T cell activation
Target Population
Young immunocompetent individuals
Care Setting
Acute hospital care
Key Highlights
Severe EBV reactivation can lead to life-threatening complications beyond HLH.
Patient presented with high fever, severe leukopenia, hyperinflammatory shock, and myocardial injury.
Elevated CD3+CD8+ T cells and inflammatory cytokines were observed.
Rapid improvement with glucocorticoids and ganciclovir treatment.
Differentiation from HLH is crucial for appropriate management.
Guideline-Based Recommendations
Diagnosis
Consider EBV reactivation in patients with unexplained severe inflammatory syndromes.
Management
Initiate glucocorticoids and antiviral therapy in severe EBV reactivation cases.
Monitoring & Follow-up
Monitor inflammatory markers and cardiac injury indicators.
Risks
Risk of misdiagnosis due to nonspecific clinical features.
Patient & Prescribing Data
Young adults with severe EBV reactivation
Glucocorticoids and ganciclovir can lead to rapid resolution of symptoms.
Clinical Best Practices
Recognize atypical manifestations of EBV reactivation.
Differentiate EBV reactivation from HLH and other severe conditions.
Provide individualized treatment based on immunophenotypic profiles.