Clinical Scorecard: Utilizing Navigated Intraoperative Ultrasound for Brainshift Correction to Enhance Decision-Making in Glioma Surgery
At a Glance
Category
Detail
Condition
Brainshift during glioma surgery affecting neuronavigation accuracy
Key Mechanisms
Brainshift causes deformation of brain tissue violating rigid body assumptions, leading to navigation errors; corrected using navigated intraoperative ultrasound fused with preoperative MRI
Target Population
Patients undergoing intra-axial brain tumor surgeries, including glioma resection and other targeted procedures like biopsy or catheter placement
Care Setting
Intraoperative neurosurgical setting with neuronavigation and ultrasound integration
Key Highlights
Brainshift is a dynamic, multifactorial process causing spatial discrepancies between preoperative imaging and actual anatomy during surgery.
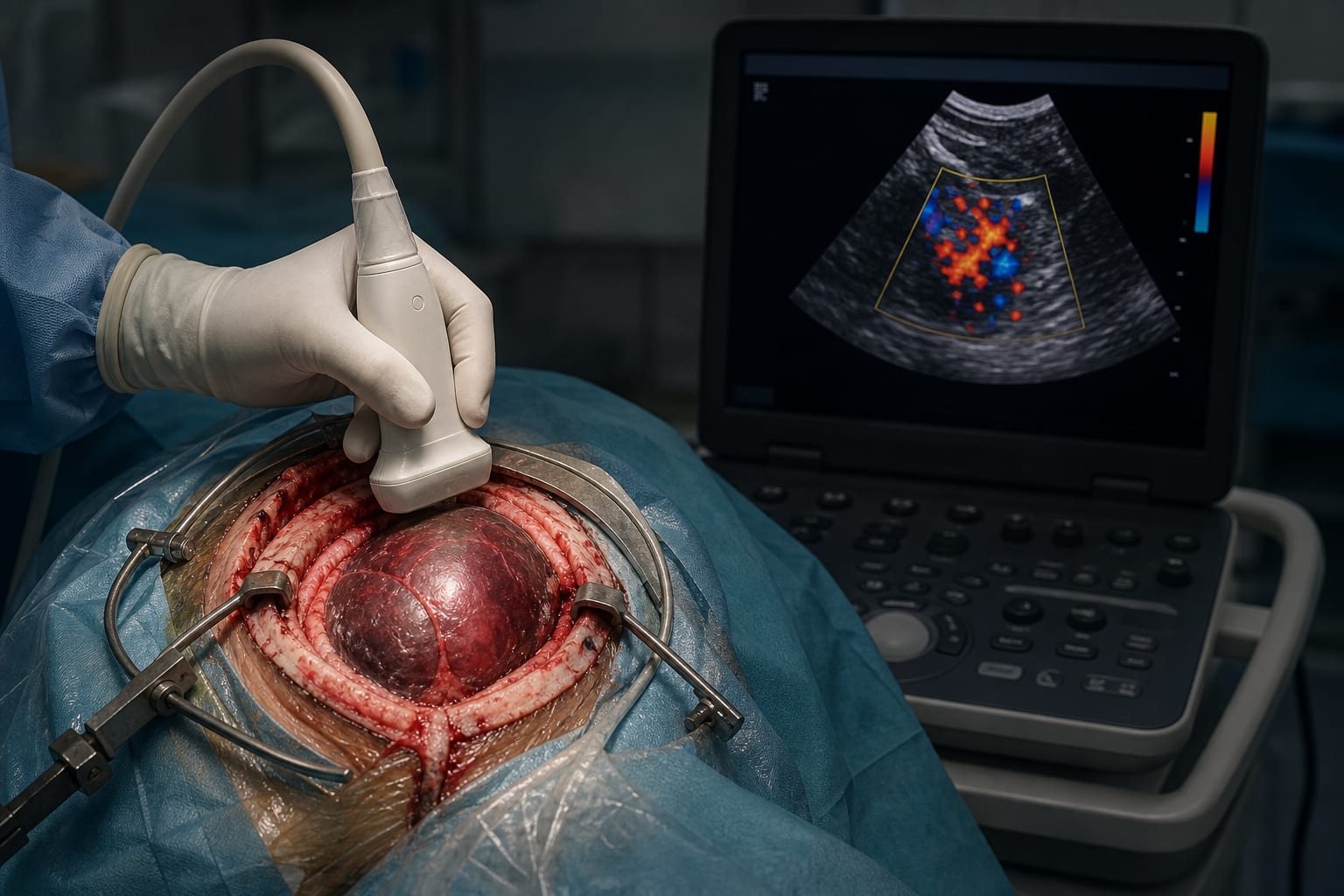
Navigated intraoperative ultrasound (iUS) fused with preoperative MRI enables real-time brainshift detection and correction via rigid image fusion.
Use of 3D navigated ultrasound and commercial brainshift correction software improves accuracy in tumor resection and preservation of eloquent structures like corticospinal tracts.
Guideline-Based Recommendations
Diagnosis
Use preoperative MRI with tractography for surgical planning and neuronavigation setup.
Employ intraoperative ultrasound fused with MRI to detect and quantify brainshift at multiple surgical stages.
Management
Apply rigid image fusion-based brainshift correction (e.g., Snap to MRI) during surgery to realign ultrasound and MRI images.
Repeat intraoperative ultrasound scans as needed to monitor and correct brainshift throughout tumor resection.
Use subcortical motor mapping to verify functional anatomy after brainshift correction.
Monitoring & Follow-up
Perform serial intraoperative ultrasound scans before dural opening, after dural opening, and after resection completion.
Qualitatively assess fusion accuracy using transparency adjustments and 'spyglass' function to evaluate landmark correspondence.
Risks
Inaccurate neuronavigation due to uncorrected brainshift may lead to incomplete tumor resection or damage to critical eloquent brain structures.
Elastic deformations are challenging to correct and may limit the precision of brainshift compensation.
Patient & Prescribing Data
Patients with intra-axial brain tumors undergoing resection with neuronavigation
Navigated intraoperative ultrasound allows dynamic brainshift correction improving surgical accuracy and functional preservation; cost-effective compared to intraoperative MRI.
Clinical Best Practices
Integrate preoperative MRI and tractography data into neuronavigation systems prior to surgery.
Acquire high-quality, wide-field 3D intraoperative ultrasound images at multiple surgical stages.
Use rigid image fusion software to correct brainshift and verify alignment with anatomical landmarks.
Combine brainshift correction with functional mapping techniques to ensure preservation of eloquent brain areas.
Repeat brainshift assessment and correction as needed during surgery to maintain navigation accuracy.