Clinical Scorecard: Advancements in Revascularization Techniques for High-Risk Pulmonary Embolism: Insights from a Single-Center Physiological Approach
At a Glance
Category
Detail
Condition
Key Mechanisms
Target Population
Patients with high-risk PE, particularly those over 75 years with underlying cardiopulmonary disease and proximal deep vein thrombosis.
Care Setting
Key Highlights
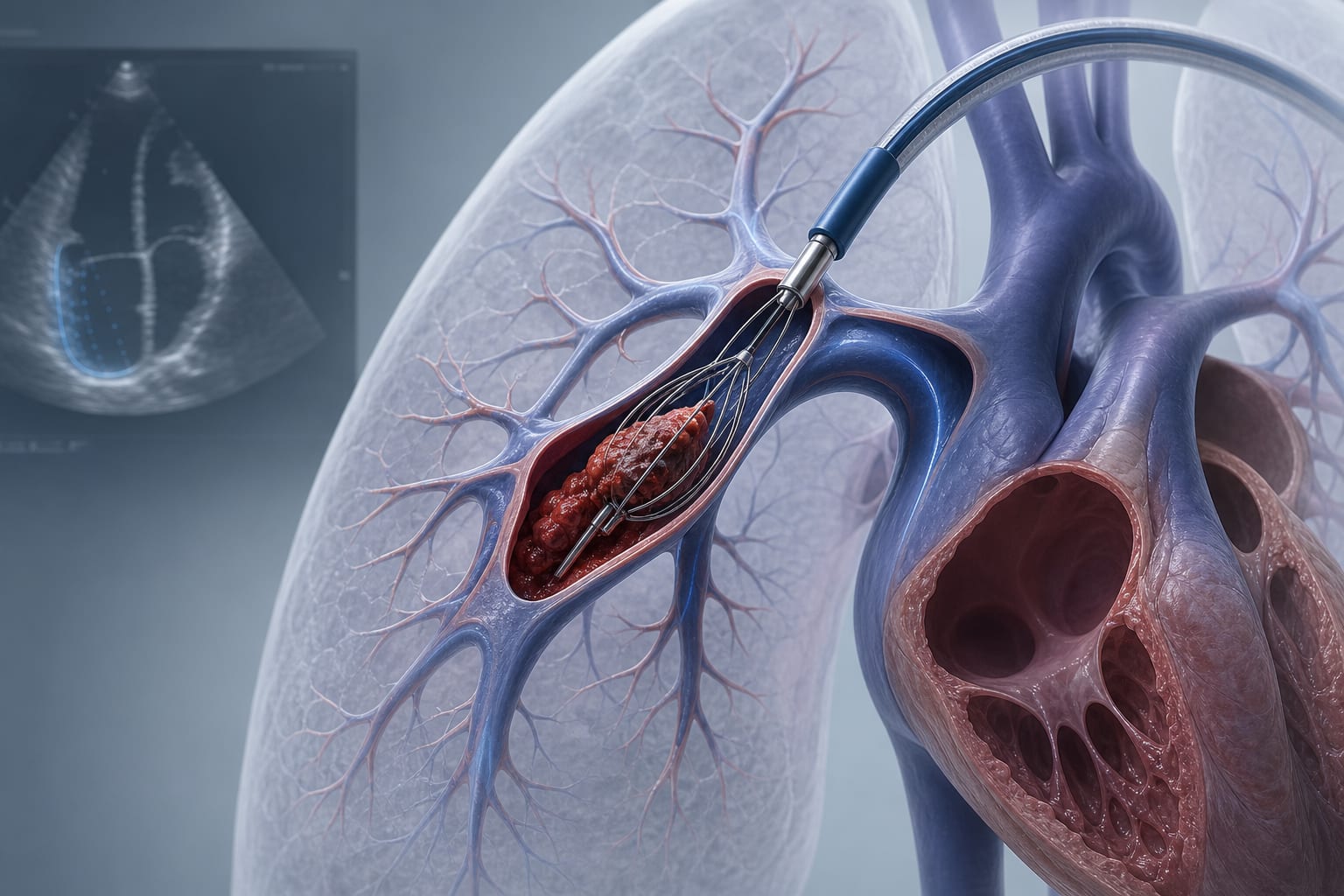
Transition from systemic thrombolysis to catheter-directed therapies (CDT) and mechanical thrombectomy.
Importance of physiologic assessment including right ventricular function and pulmonary artery pressures.
Development of a pulmonary embolism response team (PERT) for improved care coordination.
Integration of artificial intelligence for early recognition of high-risk PE cases.
Recognition of clinical classification system (Categories A–E) for patient risk stratification.
Understanding device-specific risks and optimal patient selection.
Guideline-Based Recommendations
Diagnosis
Utilize clinical classification system to identify patients at risk for deterioration.
Management
Consider selective use of reperfusion therapies based on clinical context and institutional expertise.
Monitoring & Follow-up
Monitor for signs of hemodynamic instability and RV function.
Risks
Be aware of bleeding risks associated with systemic thrombolysis, particularly in elderly patients.
Consider the use of IVC filters in unstable patients with proximal DVT.
Patient & Prescribing Data
Reduced-dose thrombolysis may be employed to mitigate bleeding risk, especially in patients over 75 years.
Clinical Best Practices
Employ multidisciplinary systems of care for managing high-risk PE.
Utilize temporary IVC filters selectively in unstable patients with proximal DVT.
Ensure careful patient selection and awareness of bleeding risks in elderly patients.