Clinical Scorecard: Ultrasound Biomicroscopy Observations in Cases of Uveitic Hypotony: A Report of Three Patients
At a Glance
Category
Detail
Condition
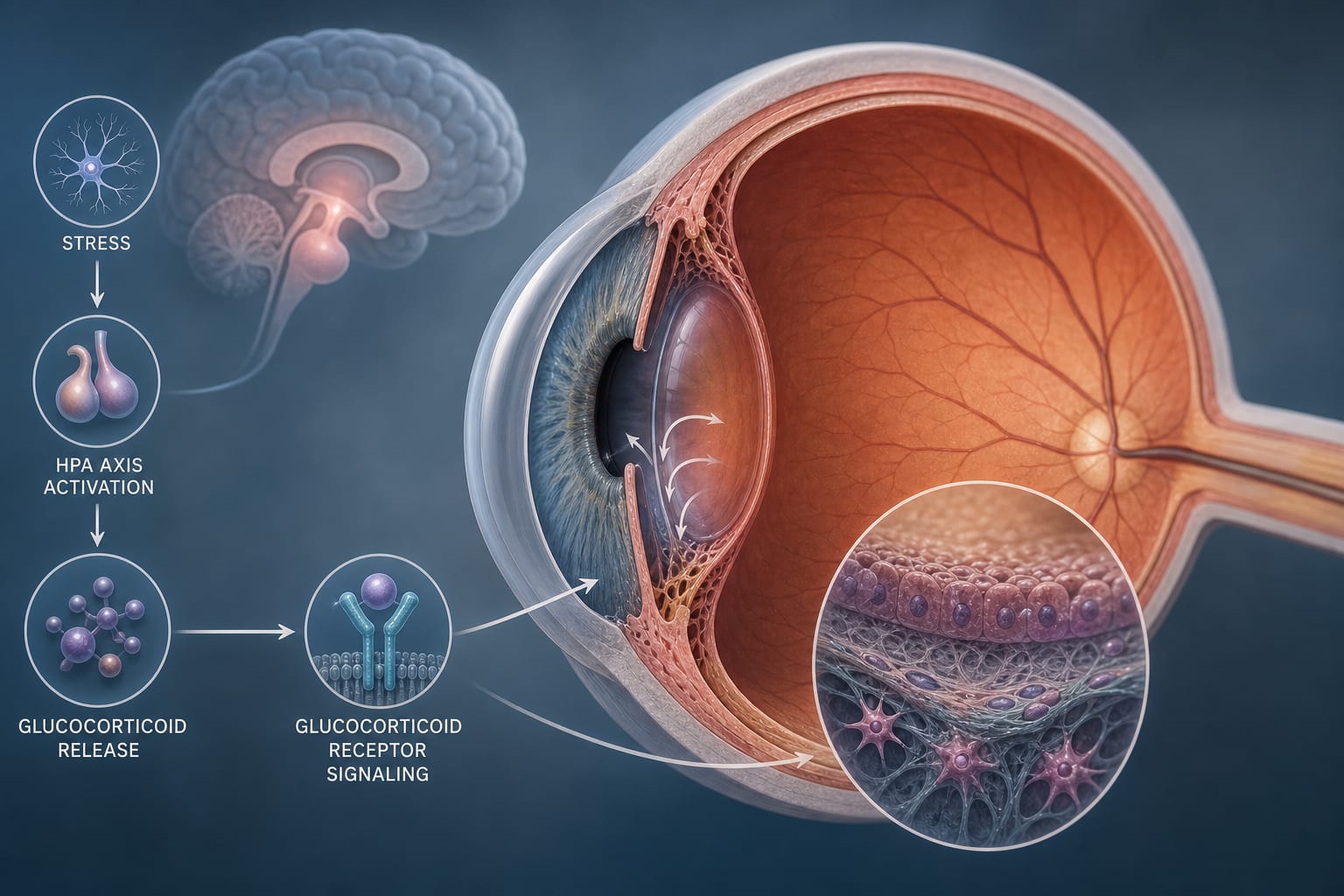
Uveitic hypotony, a serious complication of uveitis characterized by low intraocular pressure
Key Mechanisms
Acute uveitis causes transient hypotony via prostaglandin-mediated increased uveoscleral outflow; chronic uveitis leads to cyclitic membranes causing ciliary body detachment and aqueous production reduction
Target Population
Predominantly young patients with chronic or acute uveitis
Care Setting
Ophthalmology clinics and surgical centers with access to ultrasound biomicroscopy
Key Highlights
UBM provides high-resolution imaging of anterior and intermediate ocular segments, enabling visualization of cyclitic membranes and ciliary body detachment in uveitic hypotony.
Cyclitic membranes are fibrovascular proliferations causing ciliary body traction, detachment, and reduced aqueous humor production, often leading to chronic hypotony and phthisis bulbi.
UBM assists in surgical planning by delineating membrane extent and guiding safe entry points for interventions; acute hypotony has better prognosis than chronic hypotony with cyclitic membranes.
Guideline-Based Recommendations
Diagnosis
Use ultrasound biomicroscopy to evaluate ciliary body, pars plana, and cyclitic membranes when clinical examination is limited by media opacities.
Consider B-scan ultrasonography for posterior segment assessment including retina and choroid in hypotony cases.
Management
Administer systemic corticosteroids in acute uveitic hypotony to reduce inflammation.
Perform cataract extraction combined with cyclitic membrane removal and scleral indentation in chronic cases to prevent or manage hypotony.
Vitrectomy with viscoelastic injection and silicone oil tamponade may be indicated in cases with retinal detachment and severe hypotony.
Monitoring & Follow-up
Monitor intraocular pressure and visual acuity regularly post-treatment.
Use UBM imaging to assess anatomical changes and response to therapy over time.
Risks
Chronic hypotony with cyclitic membranes increases risk of maculopathy and phthisis bulbi.
Surgical interventions may not always restore aqueous flow due to persistent fibrovascular obstruction.
Loss to follow-up and complications such as phthisis bulbi can occur despite treatment.
Patient & Prescribing Data
Young adults with acute or chronic uveitis complicated by hypotony
Systemic corticosteroids are effective in acute inflammation; surgical removal of cyclitic membranes may improve outcomes but prognosis is guarded in chronic cases
Clinical Best Practices
Employ UBM for detailed assessment of anterior and intermediate segment structures in uveitic hypotony.
Individualize treatment based on disease stage and anatomical findings from imaging.
Combine corticosteroid therapy with surgical intervention when indicated to address both inflammation and structural causes.
Recognize limitations of clinical examination in presence of media opacities and rely on imaging adjuncts.
Counsel patients regarding prognosis, especially in chronic hypotony with cyclitic membrane formation.
The promise of robotic cataract surgery has been floating through the halls of ophthalmology meetings for years, and it appears the promise is now on its way to reality.