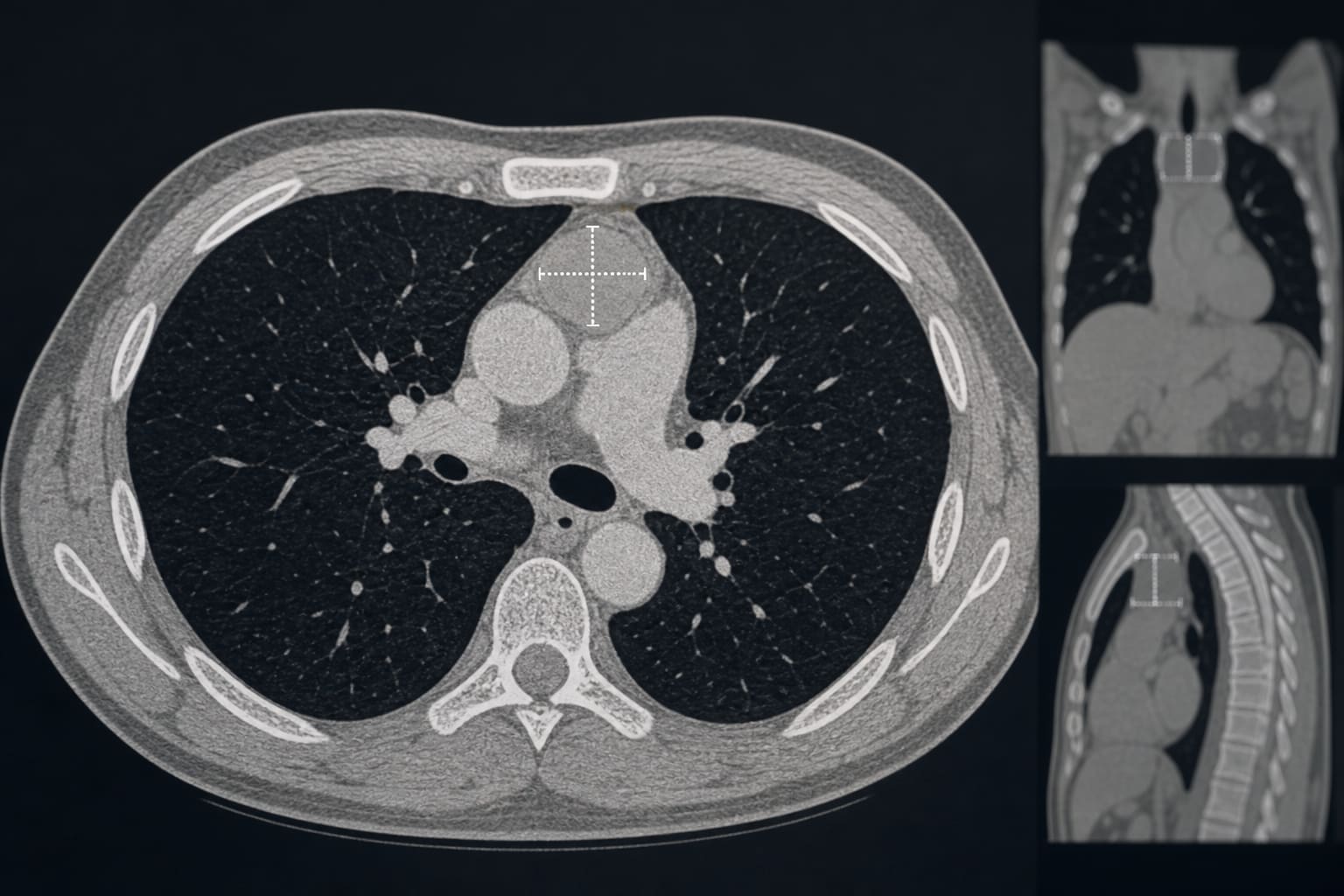
Conservative management of < 3cm anterior mediastinal lesions in lung cancer screening is safe
-
By
-
Amyn Bhamani
-
Chuen R. Khaw
-
Ruth Prendecki
-
Priyam Verghese
-
Andrew Creamer
-
Jennifer L. Dickson
-
Carolyn Horst
-
Helen Hall
-
Sophie Tisi
-
Monica Mullin
-
Tanya Patrick
-
John McCabe
-
Anne-Marie Hacker
-
Laura Farrelly
-
Esther Arthur-Darkwa
-
Neal Navani
-
Anand Devaraj
-
Allan Hackshaw
-
Arjun Nair
-
Sam M. Janes
-
July 4, 2026
-
0 min