Percutaneous nephrostomy as a marker of clinical vulnerability in non-metastatic muscle-invasive bladder cancer: prognostic and infectious implications - Scorecard - MDSpire
Advertisement
Percutaneous nephrostomy as a marker of clinical vulnerability in non-metastatic muscle-invasive bladder cancer: prognostic and infectious implications
Clinical Scorecard: The Role of Percutaneous Nephrostomy in Assessing Clinical Vulnerability in Non-Metastatic Muscle-Invasive Bladder Cancer: Implications for Prognosis and Infection Risk
At a Glance
Category
Detail
Condition
Key Mechanisms
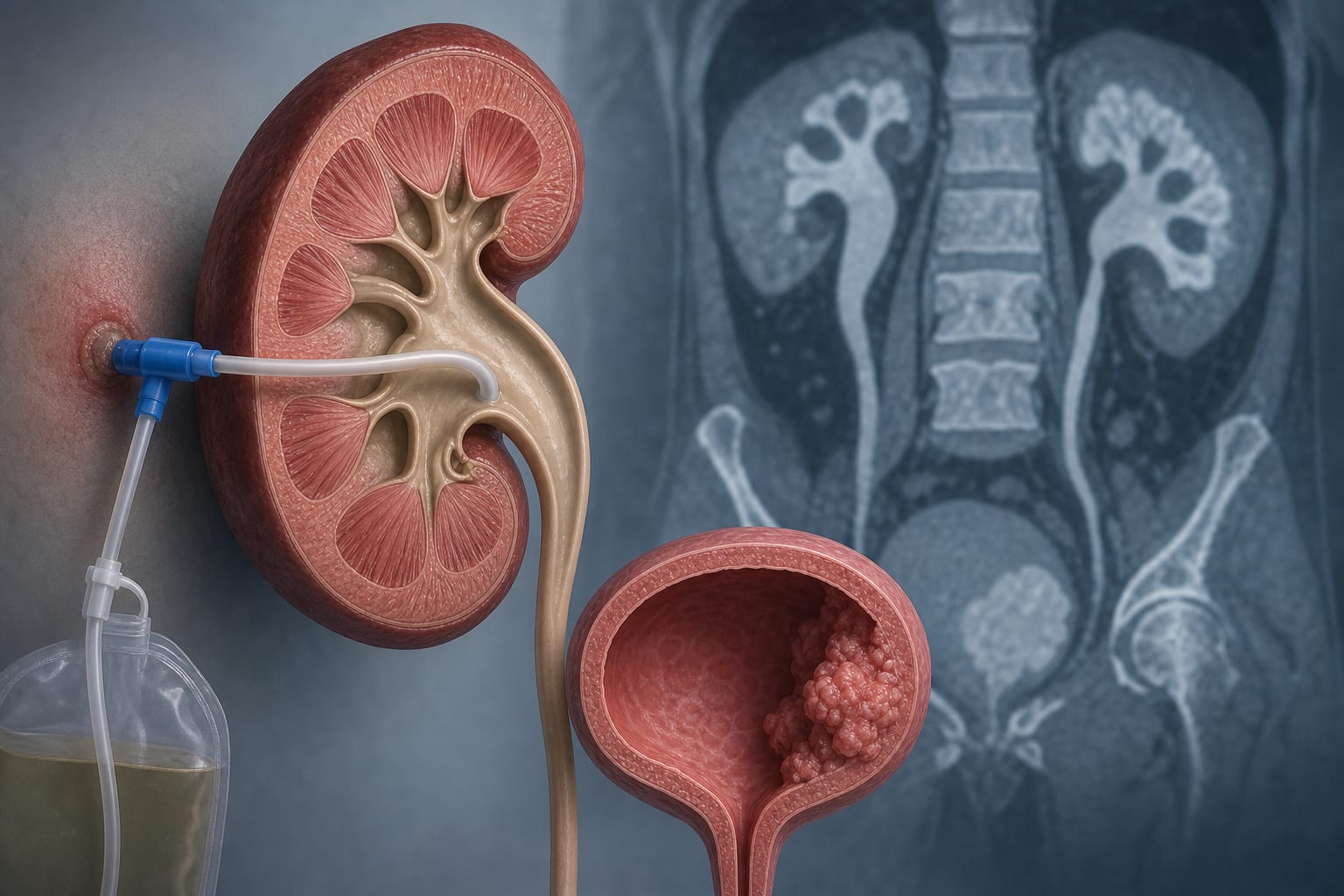
Percutaneous nephrostomy (PCN) is used to relieve malignant ureteral obstruction and is associated with increased infection risk.
Target Population
Care Setting
Key Highlights
PCN was present in 27.1% of patients with non-metastatic MIBC.
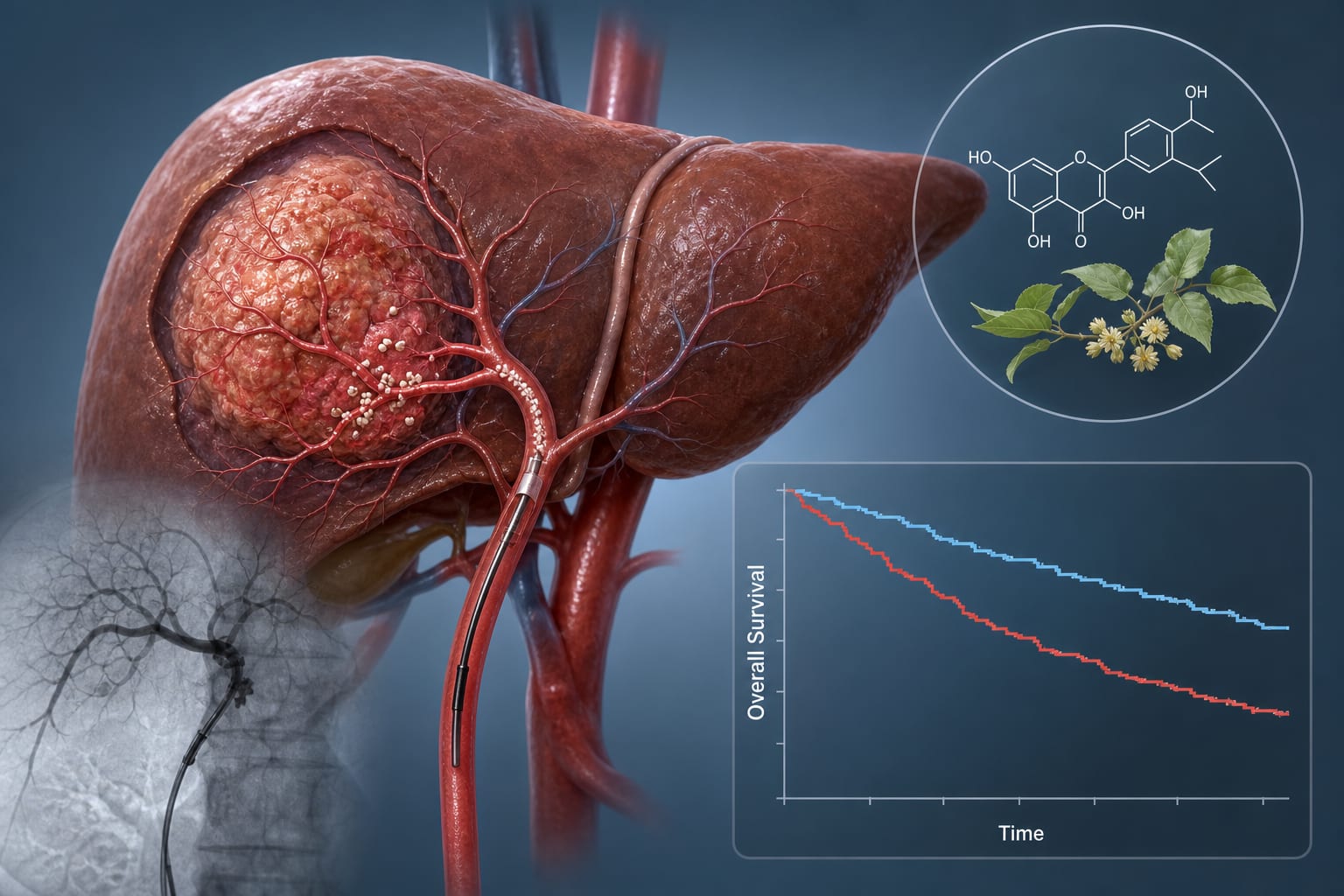
Median overall survival was shorter in the PCN group (24 months) compared to non-PCN (41 months).
PCN was independently associated with positive urine cultures and infection-related hospitalizations.
ECOG performance status, CRP, and N stage were independent predictors of overall survival.
PCN did not retain independent prognostic significance for overall survival after adjustment; however, it is a marker of clinical vulnerability.
Guideline-Based Recommendations
Diagnosis
Management
Consider multidisciplinary evaluation before PCN placement, including urologists, oncologists, and infectious disease specialists.
Monitoring & Follow-up
Risks
Patient & Prescribing Data
Adults (≥18 years) with histologically confirmed non-metastatic MIBC.
PCN may affect eligibility for neoadjuvant chemotherapy and treatment planning.
Clinical Best Practices
Evaluate clinical vulnerability before PCN placement, including comprehensive assessments of comorbidities.
Monitor for infection-related complications in patients with PCN, implementing a standardized follow-up protocol.