Retrospective clinical study of endoscopic transfrontal approach vs. transSylvian-transinsular craniotomy for hypertensive intracerebral hemorrhage in basal ganglia: efficacy comparison and value of anatomical cognition of Sylvian fissure - Scorecard - MDSpire
Advertisement
Retrospective clinical study of endoscopic transfrontal approach vs. transSylvian-transinsular craniotomy for hypertensive intracerebral hemorrhage in basal ganglia: efficacy comparison and value of anatomical cognition of Sylvian fissure
Clinical Scorecard: Comparative Analysis of Endoscopic Transfrontal Approach and TransSylvian-Transinsular Craniotomy for Hypertensive Intracerebral Hemorrhage in the Basal Ganglia: Efficacy and the Role of Sylvian Fissure Anatomy in Surgical Outcomes
At a Glance
Category
Detail
Condition
Hypertensive Intracerebral Hemorrhage (HICH)
Key Mechanisms
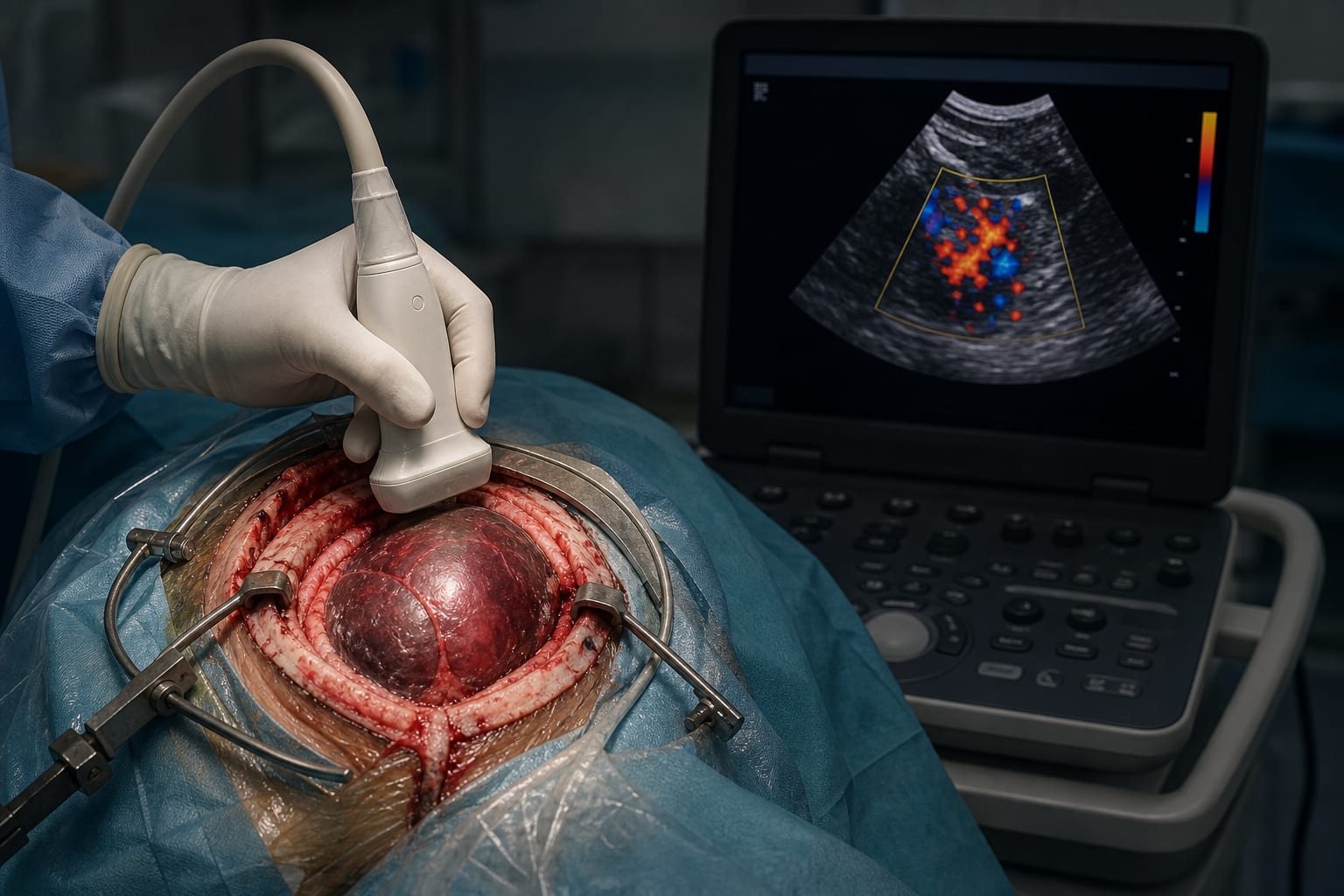
Endoscopic transfrontal surgery and transSylvian-transinsular craniotomy for hematoma evacuation.
Target Population
Adults with basal ganglia hypertensive intracerebral hemorrhage.
Care Setting
Neurosurgery department in a hospital.
Key Highlights
Endoscopic surgery showed shorter operation time and lower complication rate.
No significant differences in hematoma clearance rate and postoperative rebleeding rate between groups.
Guideline-Based Recommendations
Diagnosis
Timely and effective hematoma evacuation is important.
Management
Surgical approach should be tailored to patient-specific characteristics.
Monitoring & Follow-up
Postoperative follow-up for at least 3 months is recommended.
Risks
Consider potential complications such as rebleeding and pulmonary infection.
Patient & Prescribing Data
230 patients with basal ganglia HICH.
Endoscopic approach offers minimally invasive advantages over traditional craniotomy.