Clinical Scorecard: Collateral Mapping: Forecasting Lesion Expansion and Penumbral Area Following Acute Anterior Circulation Ischemic Stroke
At a Glance
Category
Detail
Condition
Acute ischemic stroke due to large vessel steno-occlusion in the anterior circulation
Key Mechanisms
Collateral circulation influences infarct growth and penumbral salvageability; imaging of collateral flow dynamics predicts lesion expansion
Target Population
Patients older than 18 years with acute ischemic stroke due to occlusion or severe stenosis of the internal carotid artery and/or M1 or M2 segment of the middle cerebral artery
Care Setting
Acute stroke care in hospital settings with advanced neuroimaging capabilities
Key Highlights
Follow-up infarct volume is a strong independent predictor of functional outcome after recanalization treatments.
Perfusion imaging using Tmax > 6 s threshold tends to overestimate penumbra volume, affecting patient selection.
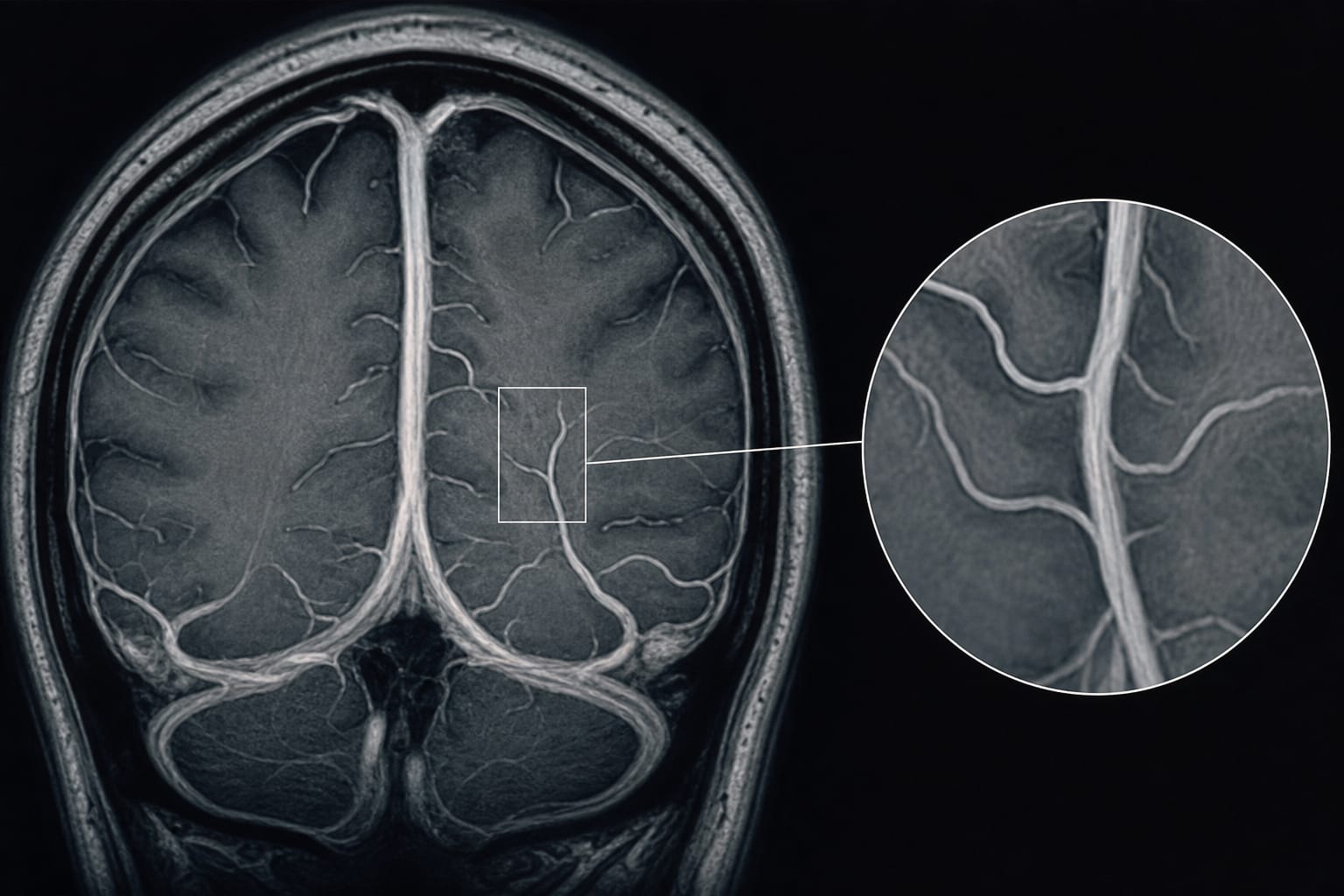
Collateral mapping via dynamic contrast-enhanced MR angiography provides dynamic tissue-level information to better predict lesion growth and penumbra extent.
Guideline-Based Recommendations
Diagnosis
Use CT or MR perfusion imaging with caution for penumbra estimation due to overestimation risks.
Employ collateral circulation imaging (collateral maps) derived from dynamic contrast-enhanced MR angiography to assess collateral status and predict lesion growth.
Assess stroke severity with NIHSS and functional outcome with modified Rankin scale at 90 days.
Management
Select patients for recanalization treatments based on accurate penumbra assessment incorporating collateral status.
Consider intravenous thrombolysis and intraarterial thrombectomy where appropriate, noting that poor collaterals may limit benefit.
Exclude patients with premorbid modified Rankin scale > 2, hemorrhagic transformation, or procedure-related complications from certain interventions.
Monitoring & Follow-up
Perform follow-up diffusion-weighted imaging within 7 days to evaluate lesion volume and growth.
Monitor collateral perfusion status dynamically to forecast infarct expansion and adjust treatment plans accordingly.
Risks
Poor collateral circulation is associated with accelerated infarct growth, hemorrhagic complications, and unfavorable functional outcomes even after successful recanalization.
Overestimation of penumbra by perfusion imaging may lead to inappropriate patient selection for interventions.
Patient & Prescribing Data
Adults with acute anterior circulation large vessel occlusion ischemic stroke evaluated within 8 hours of symptom onset
Collateral mapping can improve selection for recanalization therapies by better predicting salvageable brain tissue and lesion growth, potentially improving functional outcomes.
Clinical Best Practices
Incorporate collateral circulation imaging using dynamic contrast-enhanced MR angiography to complement perfusion imaging for penumbra assessment.
Use lesion growth ratio (follow-up lesion volume to baseline lesion volume) ≥ 1.2 to define significant lesion growth considering vasogenic edema.
Evaluate functional outcomes at 90 days using modified Rankin scale to guide prognosis and rehabilitation planning.
by Jin Seok Yi, Hee Jong Ki, Yoo Sung Jeon, Jeong Jin Park, Taek-Jun Lee, Jin Tae Kwak, Sang Bong Lee, Hyung Jin Lee, In Seong Kim, Joo Hyun Kim, Ji Sung Lee, Hong Gee Roh, Hyun Jeong Kim