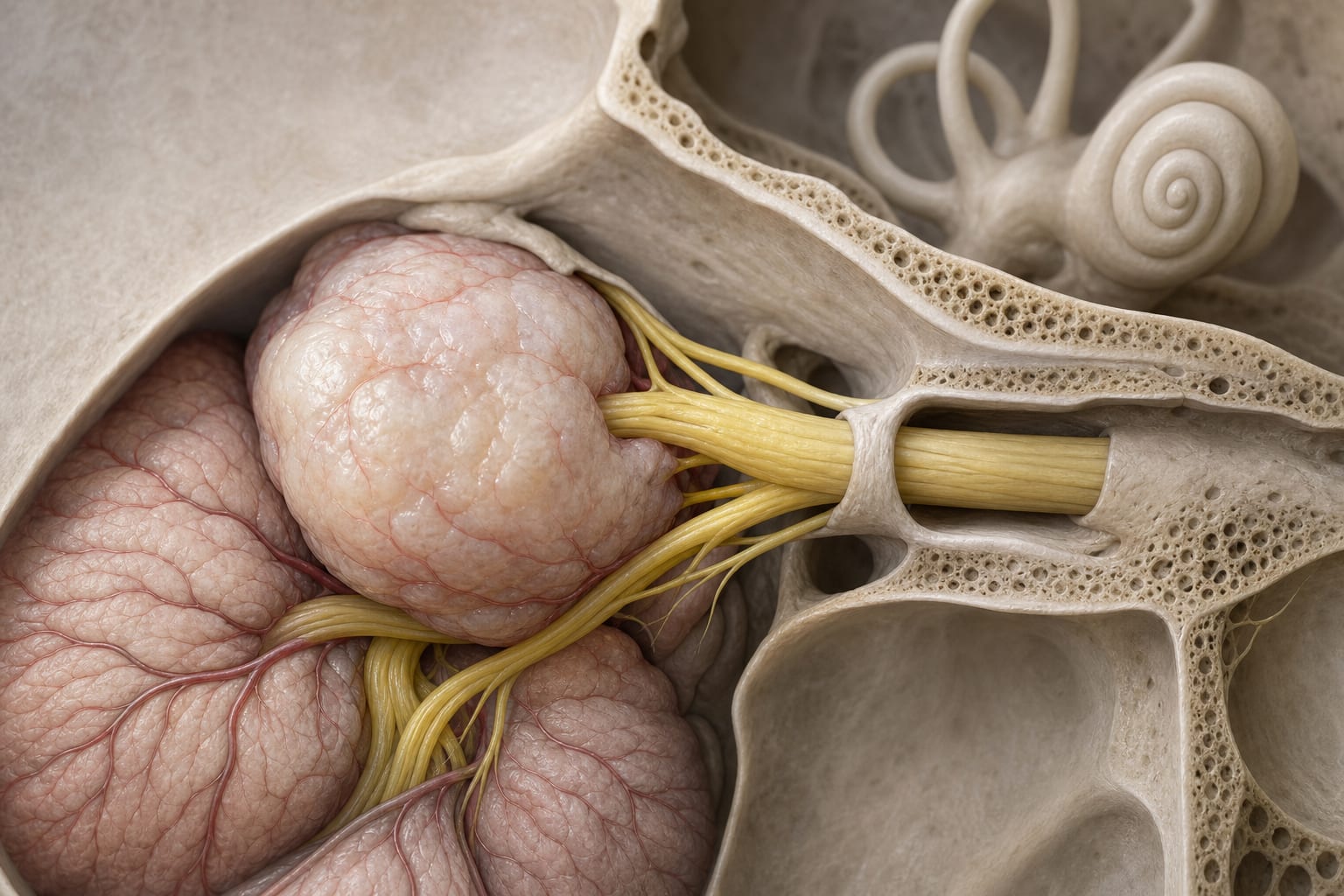
A Single-center experience of subperineural resection of intracranial schwannomas and the clinical course following subtotal resection
By
Azuna Tomioka
Ryota Tamura
Junki Sogano
Kosuke Karatsu
Konosuke Ishikawa
Taichi Sayanagi
Takenori Akiyama
Ryo Ueda
Masahiro Toda
June 24, 2026
Clinical Scorecard: Clinical Outcomes Following Subperineural Resection of Intracranial Schwannomas: Insights from a Single-Center Study
At a Glance
Category Detail
Condition Intracranial Schwannomas Key Mechanisms Subperineural resection technique for tumor removal and neurological function preservation. Target Population Patients with intracranial schwannomas, including vestibular and non-vestibular types. Care Setting Single-center surgical evaluation.
Key Highlights
Total resection rates varied by cranial nerve origin, with CN VIII schwannomas showing a 70.3% TR rate. Postoperative regrowth occurred in 27.3% of CN VIII and 57.1% of CN V subtotal resection cases. Retreatment was required in 4/44 CN VIII and 0/7 CN V cases. Higher regrowth rates observed in CN IX–XI (83.3%) and CN XII (66.7%) schwannomas. Optimal timing for postoperative radiotherapy after subtotal resection remains controversial. Guideline-Based Recommendations
Diagnosis
Diagnosis of schwannomas based on imaging and clinical evaluation. Management
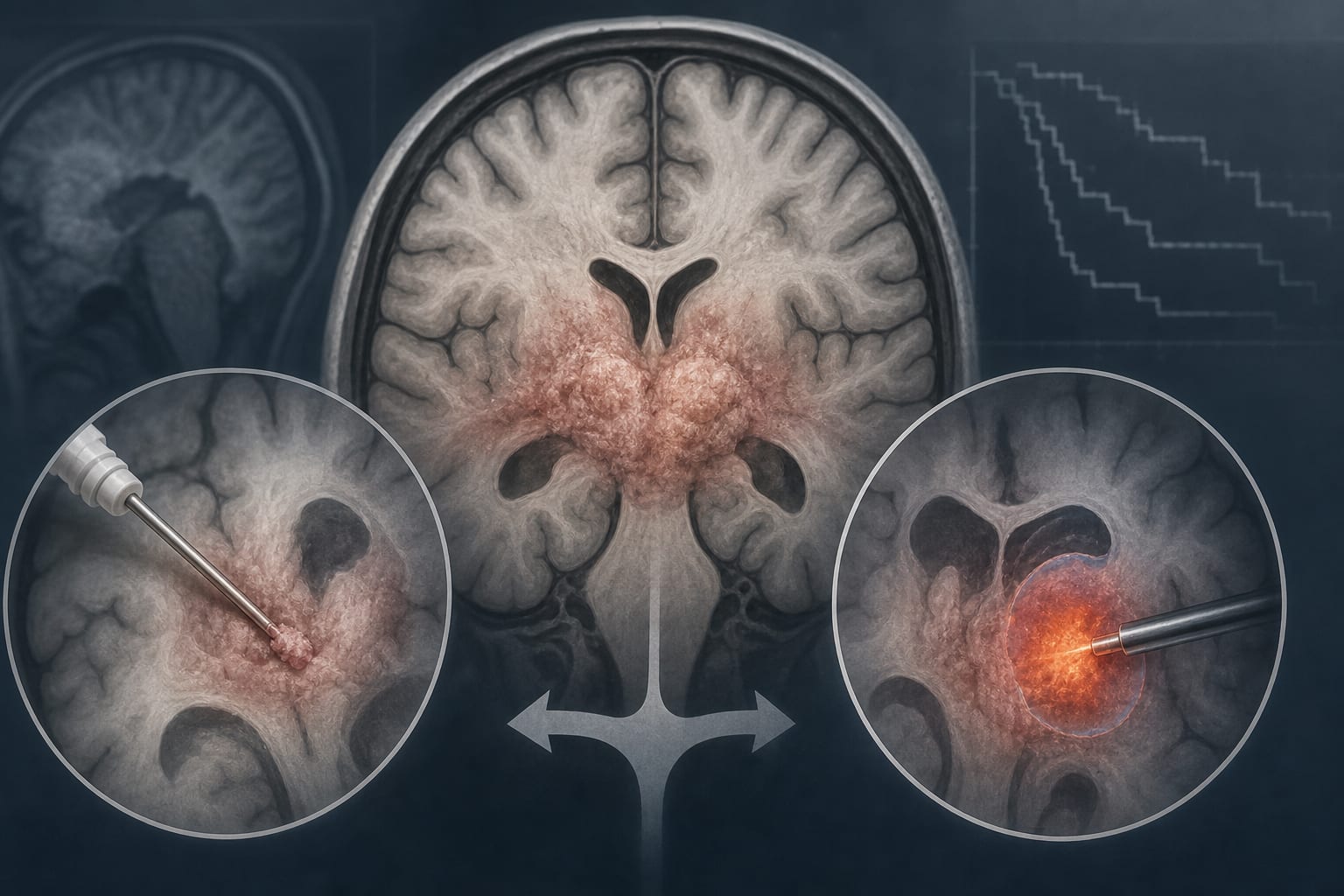
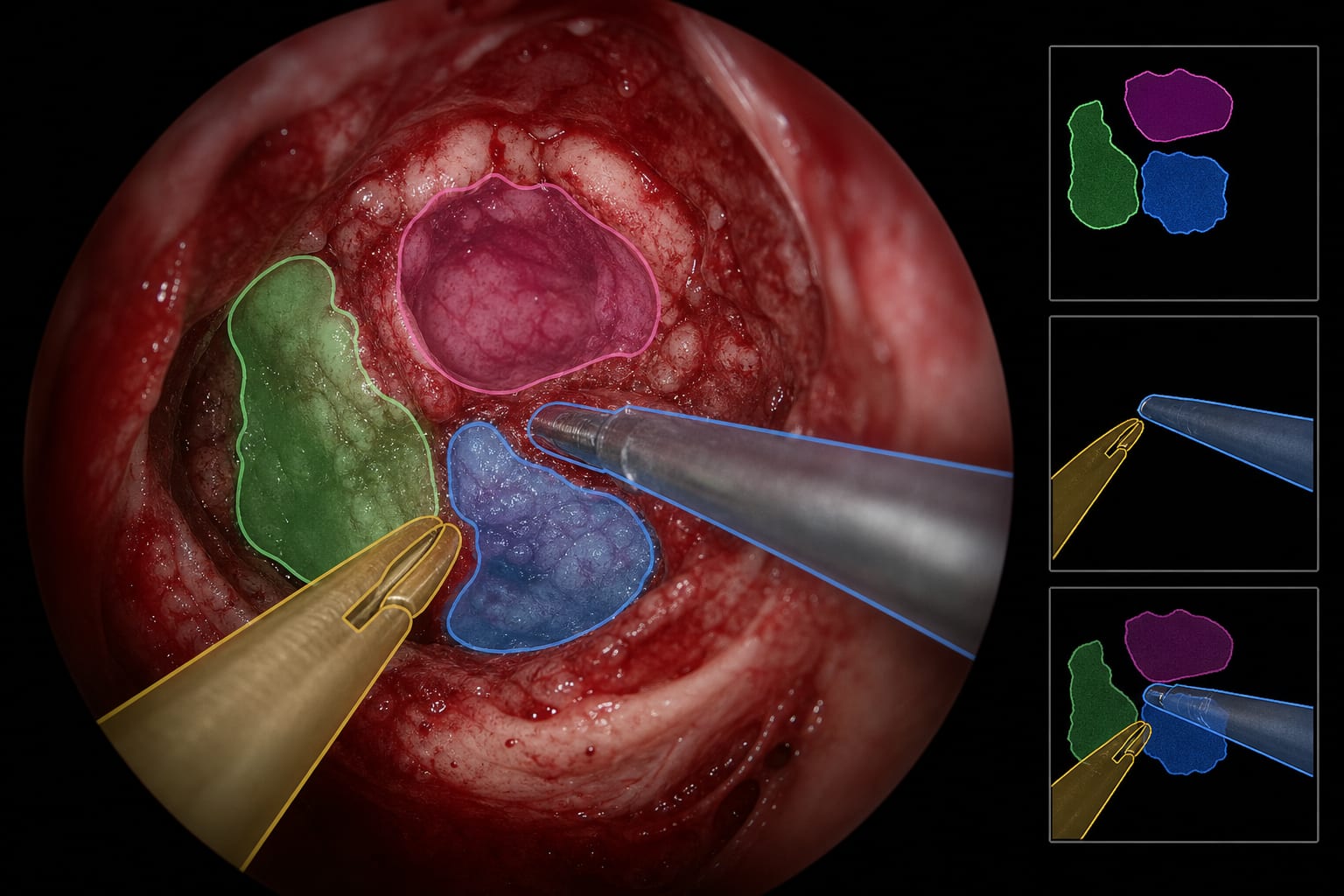
Subperineural resection is recommended for surgical management of intracranial schwannomas. Monitoring & Follow-up
Postoperative monitoring for tumor regrowth using imaging. Risks
Risks include incomplete resection and potential for tumor regrowth. Patient & Prescribing Data
186 patients with intracranial schwannomas.
Subperineural resection technique applied consistently across all cases.
Clinical Best Practices
Utilize intraoperative monitoring to preserve neurological function. Assess facial and auditory function postoperatively using standardized scales. Consider individual cranial nerve origin when evaluating surgical outcomes. Related Resources & Content