The association of remnant cholesterol inflammatory index with the risk of major adverse cardiovascular events in patients with angina undergoing percutaneous coronary intervention: a retrospective study - Scorecard - MDSpire
Advertisement
The association of remnant cholesterol inflammatory index with the risk of major adverse cardiovascular events in patients with angina undergoing percutaneous coronary intervention: a retrospective study
Clinical Scorecard: Linking the Remnant Cholesterol-Inflammation Index to Major Adverse Cardiovascular Event Risk in Angina Patients Undergoing Percutaneous Coronary Intervention: A Retrospective Analysis
At a Glance
Category
Detail
Condition
Angina and Major Adverse Cardiovascular Events (MACE)
Key Mechanisms
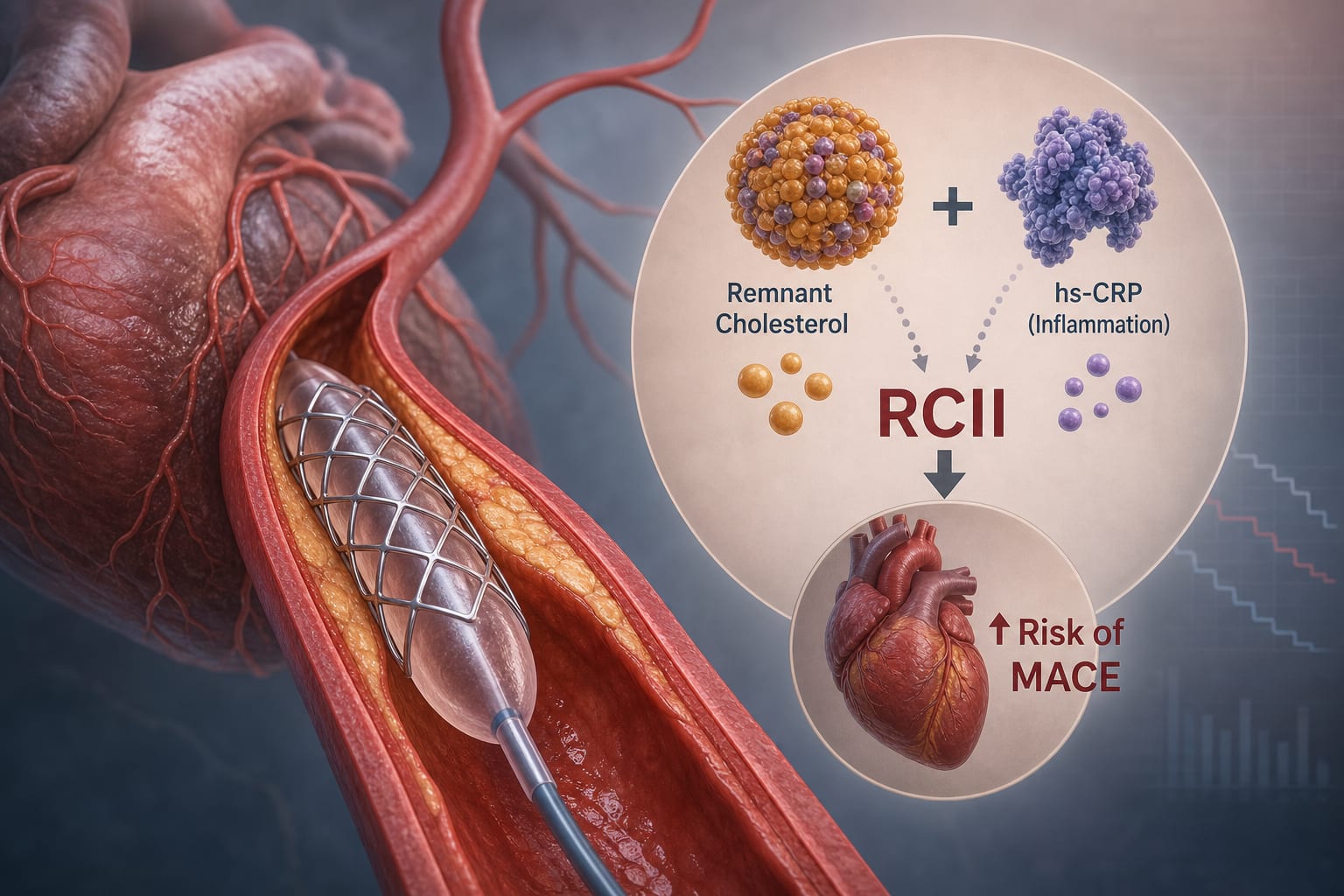
Remnant cholesterol (RC) and high-sensitivity C-reactive protein (hs-CRP) reflect metabolic and inflammatory risks.
Target Population
Patients with angina undergoing percutaneous coronary intervention (PCI)
Care Setting
Cardiology
Key Highlights
Study included 2,171 angina patients with a median follow-up of 36 months.
Each standard deviation increase in RCII was associated with a 5% higher MACE risk.
Moderate discriminatory ability of RCII for MACE risk was demonstrated with AUCs ranging from 0.739 to 0.786 over 30 months.
RCII significantly associated with MACE risk across various subgroups including age, sex, and comorbidities.
RCII may serve as a potential clinical biomarker for assessing MACE risk.
Guideline-Based Recommendations
Diagnosis
Evaluate baseline RCII in patients with angina undergoing PCI.
Management
Consider RCII as a potential biomarker for cardiovascular risk assessment.
Monitoring & Follow-up
Monitor RCII levels to evaluate ongoing cardiovascular risk.
Risks
Patients with elevated RCII may have increased risk of MACE.
Patient & Prescribing Data
Angina patients undergoing PCI.
Focus on managing both dyslipidemia and inflammation to reduce MACE risk.
Clinical Best Practices
Incorporate RCII measurement in routine risk assessment for angina patients.
Address both metabolic and inflammatory factors in cardiovascular risk management.
Federal prosecutors allege that a Florida physician and research staff fabricated clinical trial records that were submitted into database systems used to evaluate investigational drugs.