Clinical Scorecard: Utilization of Gastrointestinal Multiplex PCR Panel for Diagnosing Amoebic Liver Abscess: A Report on Three Pediatric Cases
At a Glance
Category
Detail
Condition
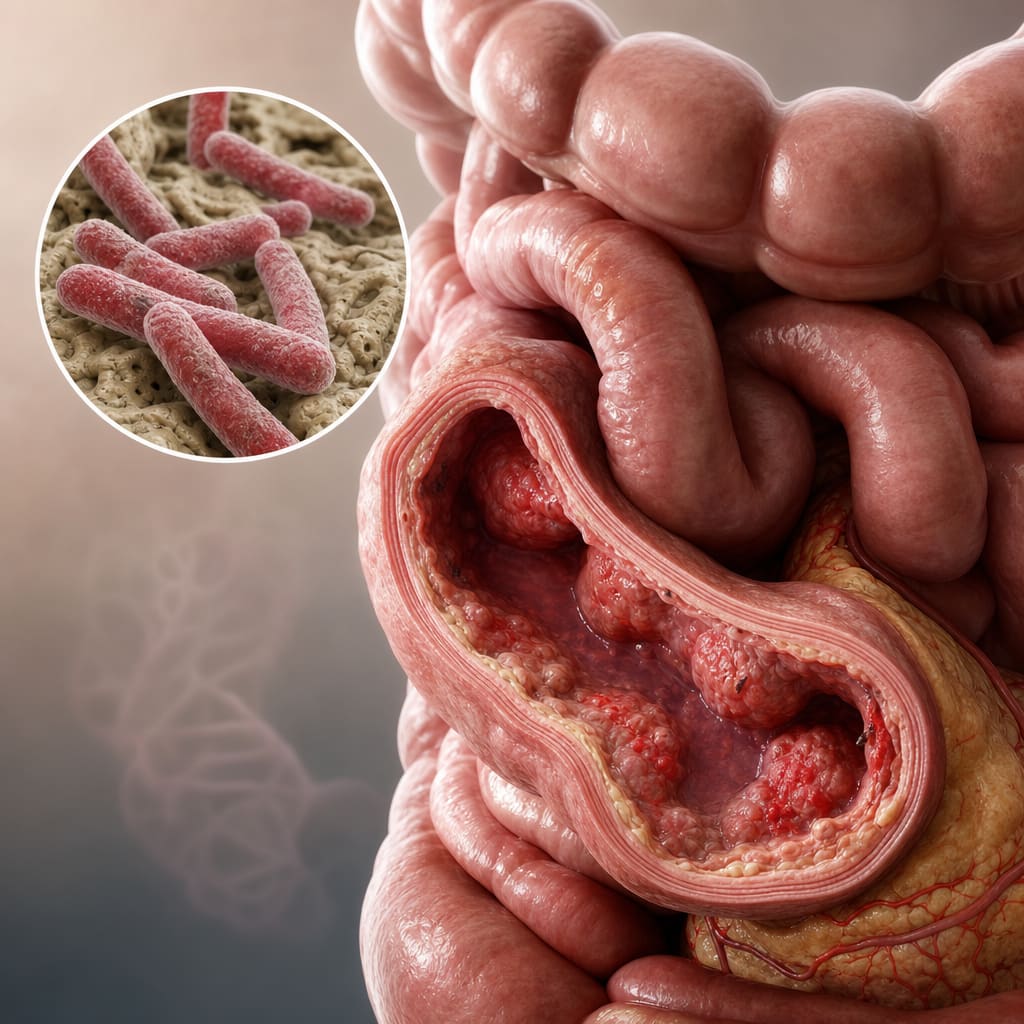
Amoebic liver abscess caused by Entamoeba histolytica
Key Mechanisms
Invasive infection by E. histolytica leading to liver abscess formation; detection of pathogen genetic material via multiplex PCR
Target Population
Pediatric patients with suspected liver abscess
Care Setting
Resource-limited, high-burden settings; hospital with imaging and surgical drainage capabilities
Key Highlights
Off-label use of FilmArray Gastrointestinal® multiplex PCR panel on liver abscess fluid enabled rapid and accurate diagnosis of E. histolytica.
Traditional diagnostic methods (immunodiagnosis, microscopy, cultures) have limitations including delayed antibody detection and false negatives.
Targeted antiamoebic therapy guided by PCR results led to favorable clinical outcomes in all three pediatric cases.
Guideline-Based Recommendations
Diagnosis
Consider amoebic liver abscess in patients with right lobe liver abscesses unresponsive to empirical antibiotics, especially with relevant epidemiological risk factors.
Use imaging (ultrasound) for lesion detection but rely on molecular diagnostics for etiological confirmation.
Employ multiplex PCR panels on liver abscess fluid as a rapid diagnostic tool, acknowledging current off-label status and need for further validation.
Management
Initiate empirical antibiotic therapy covering bacterial pathogens initially; add metronidazole when amoebic etiology is suspected.
Adjust treatment to targeted antiamoebic therapy upon confirmation of E. histolytica by PCR.
Perform surgical or percutaneous drainage for large or non-resolving abscesses.
Monitoring & Follow-up
Monitor clinical signs, inflammatory markers, and abscess size via imaging to assess treatment response.
Reassess therapy if clinical deterioration or abscess enlargement occurs.
Risks
Delayed or inaccurate diagnosis may lead to inappropriate antibiotic use and increased morbidity.
Off-label use of multiplex PCR requires cautious interpretation pending further validation.
Potential complications include intestinal necrosis, peritonitis, and toxic megacolon if untreated.
Patient & Prescribing Data
Three pediatric patients aged 17 months to 5 years with liver abscesses
Empirical broad-spectrum antibiotics were initially used; metronidazole was added upon suspicion or confirmation of amoebic infection. PCR confirmation allowed discontinuation of unnecessary antibiotics and continuation of targeted antiamoebic therapy.
Clinical Best Practices
Use multiplex PCR panels on liver abscess fluid to rapidly identify E. histolytica in suspected cases.
Combine clinical, epidemiological, and imaging data to guide suspicion and management of amoebic liver abscess.
Perform abscess drainage when indicated to obtain diagnostic material and aid treatment.
Adjust antimicrobial therapy based on molecular diagnostic results to avoid unnecessary antibiotic exposure.
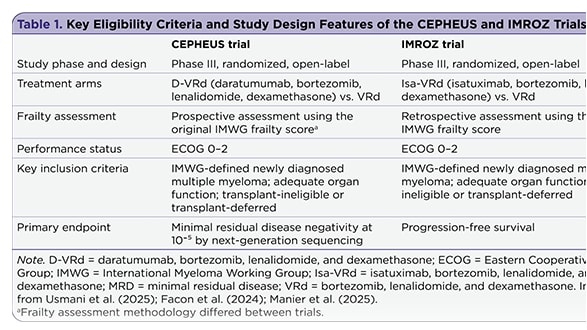
The management of newly diagnosed transplant-ineligible multiple myeloma remains challenging, in part due to the complexity of treatment decisions for frail patients. Recent subgroup analyses provide insight into whether quadruplet therapy may offer advantages over triplet therapy in this population.