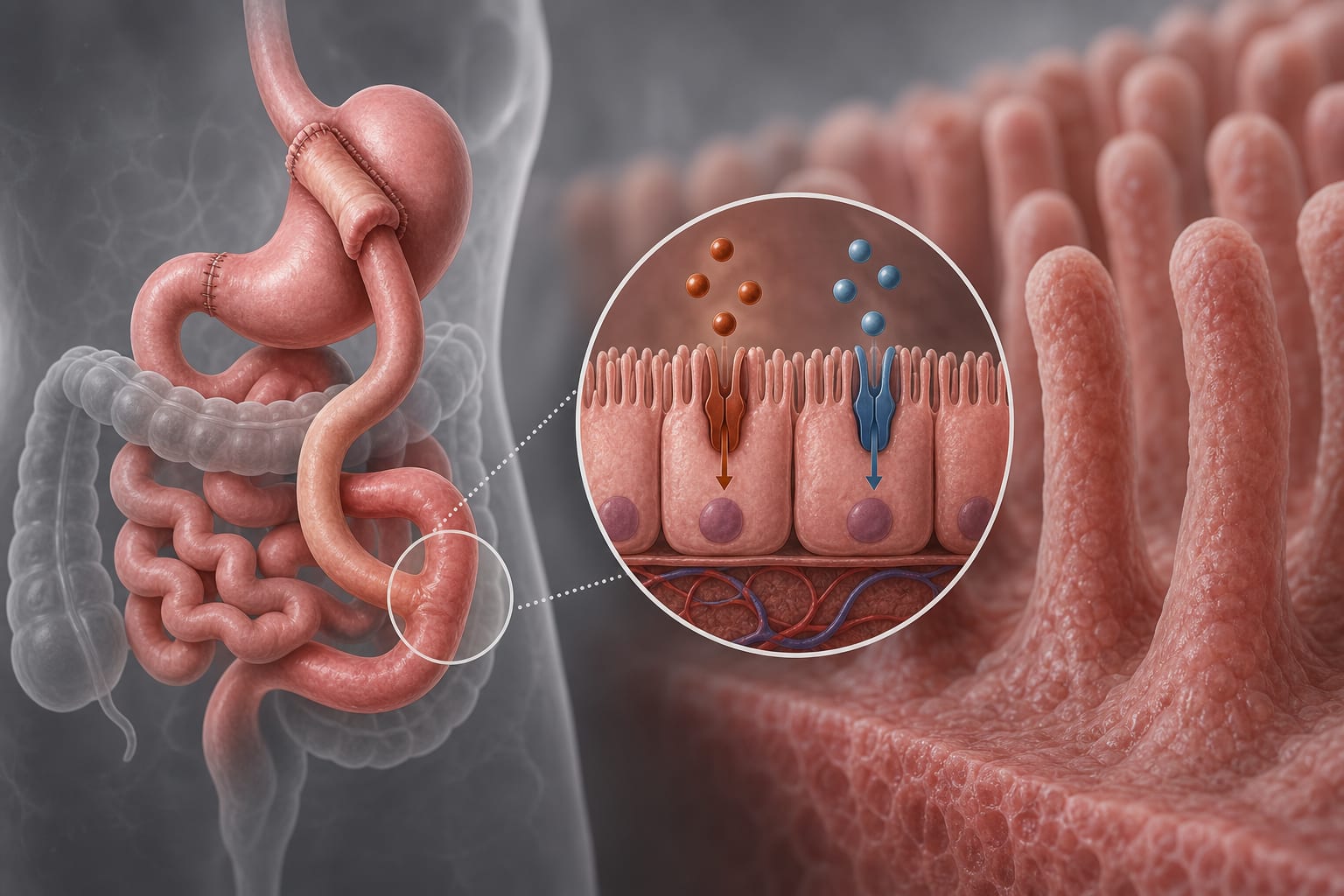
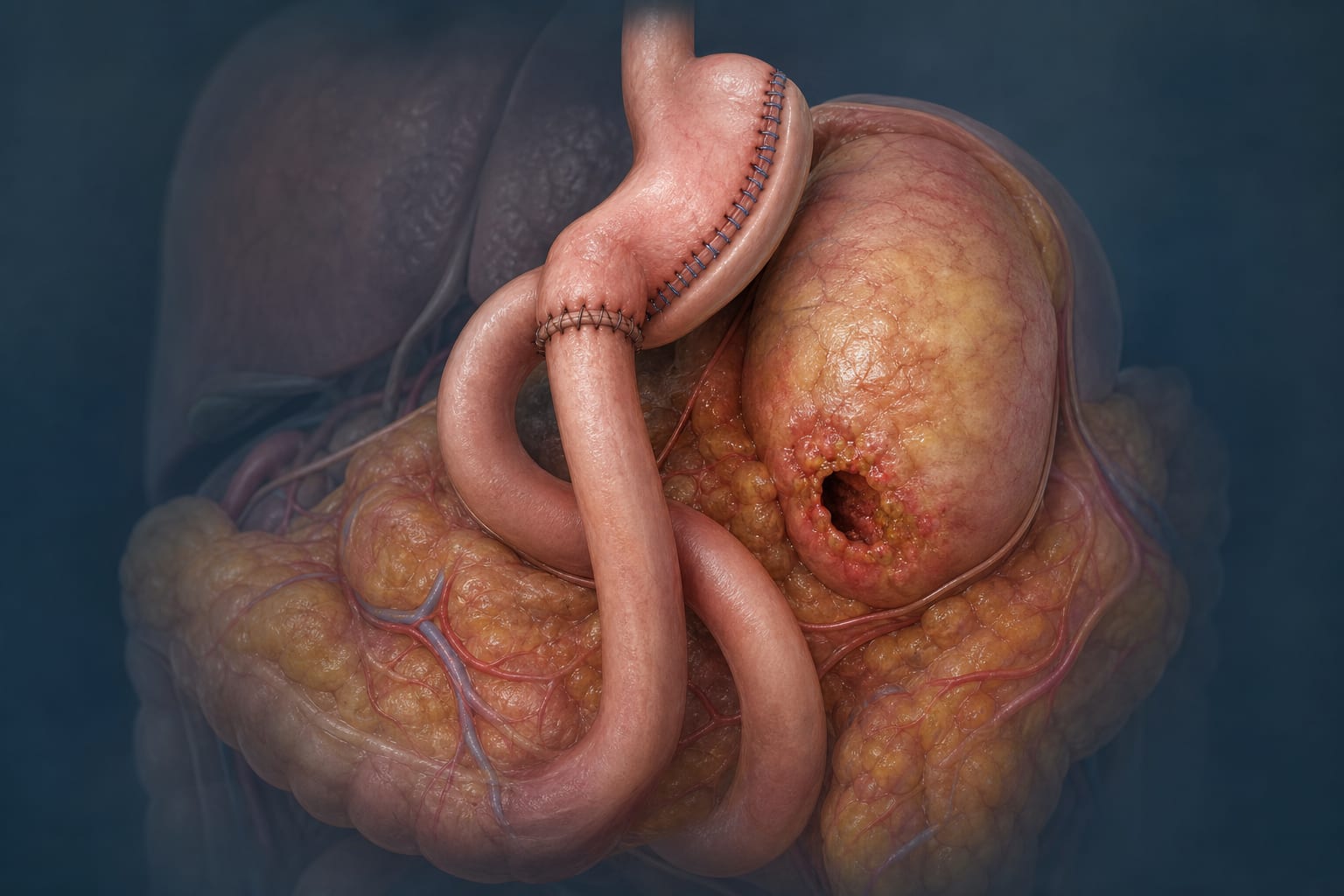
Surgical reduction of stomach size to induce weight loss and metabolic improvements
Target Population
Patients undergoing sleeve gastrectomy for obesity
Care Setting
Specialized bariatric surgical centers with long-term outpatient follow-up
Key Highlights
Sleeve gastrectomy is the most common bariatric surgery due to its technical simplicity and effectiveness.
Long-term follow-up adherence decreases significantly over time, with only 57% to 29.6% adherence after 5 to 7 years.
Older age is the only independent predictor of completing 10-year follow-up after sleeve gastrectomy.
Guideline-Based Recommendations
Diagnosis
Assess eligibility for metabolic bariatric surgery based on established criteria.
Evaluate preoperative obesity-related diseases such as type 2 diabetes and hypertension.
Management
Perform sleeve gastrectomy using standard technique with a 36 F bougie starting 4–6 cm from the pylorus.
Provide free access to outpatient clinics and direct surgeon contact to encourage follow-up.
Monitoring & Follow-up
Conduct systematic long-term postoperative follow-up to assess weight loss durability and complications.
Monitor for recurrence of obesity, remission of comorbidities, and development or persistence of GERD.
Use standardized metrics such as %EWL and %TWL for weight loss assessment.
Risks
Recognize that de novo GERD symptoms occur in approximately 42.7% of patients postoperatively.
Be aware of potential need for additional surgery in some patients.
Consider that loss to follow-up may hinder timely identification of complications.
Patient & Prescribing Data
150 patients undergoing sleeve gastrectomy with 101 completing 10-year follow-up
Older patients are more likely to adhere to long-term follow-up; median total weight loss at 10 years is approximately 21.5%; remission rates for type 2 diabetes and hypertension are 55.6% and 36.8%, respectively.
Clinical Best Practices
Encourage patient engagement through accessible outpatient services and direct communication channels.
Identify patients at risk of loss to follow-up, focusing on younger patients for targeted interventions.
Monitor and manage GERD symptoms proactively, including consideration of conversion surgery when indicated.
Use standardized reporting criteria for consistent assessment of outcomes and complications.