Culture-negative cryptogenic splenic abscess in an immunocompetent host with recurrent misdiagnosis as pleural effusion: a case report with a review of the literature - Scorecard - MDSpire
Advertisement
Culture-negative cryptogenic splenic abscess in an immunocompetent host with recurrent misdiagnosis as pleural effusion: a case report with a review of the literature
Clinical Scorecard: A Case Study of Culture-Negative Cryptogenic Splenic Abscess in an Immunocompetent Patient Misdiagnosed as Pleural Effusion: Insights from Literature Review
At a Glance
Category
Detail
Condition
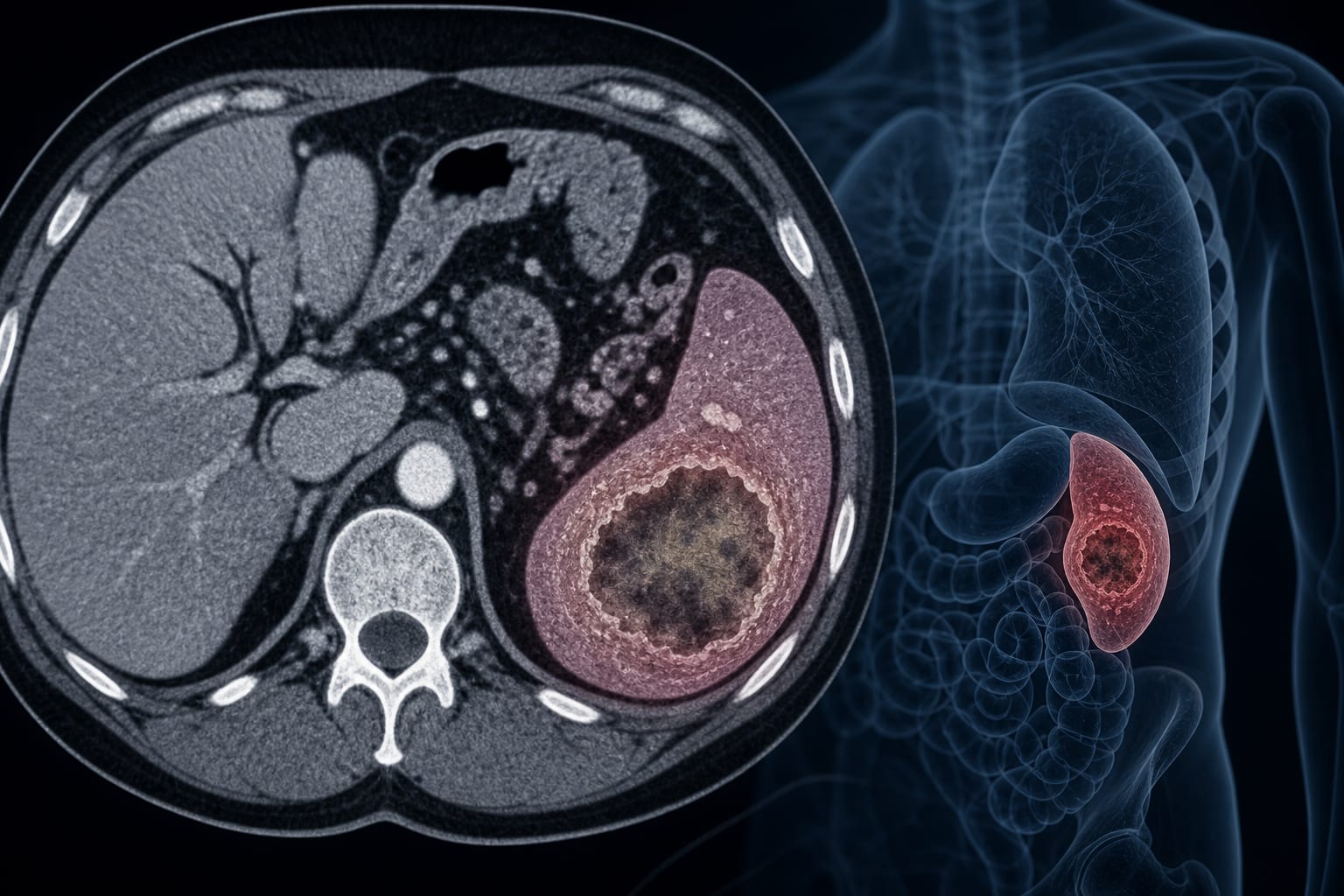
Cryptogenic Splenic Abscess
Key Mechanisms
Abscess formation through hematogenous seeding, direct extension, or post-procedural complications.
Target Population
Immunocompetent individuals without identifiable predisposing conditions.
Care Setting
Emergency department and surgical intervention.
Key Highlights
Splenic abscess can mimic pneumonia and pleuritis, leading to diagnostic delays.
Culture-negative results are common and should not delay surgical intervention.
Contrast-enhanced CT is the gold standard for diagnosis.
Empirical antibiotic therapy is critical in management.
Post-splenectomy vaccinations are necessary to prevent infections.
Guideline-Based Recommendations
Diagnosis
Utilize contrast-enhanced CT for definitive diagnosis of splenic abscess.
Management
Initiate broad-spectrum antibiotic therapy and consider surgical intervention if no improvement.
Monitoring & Follow-up
Monitor inflammatory markers and clinical symptoms to assess treatment efficacy.
Risks
Potential for misdiagnosis leading to delayed treatment and increased morbidity.
Patient & Prescribing Data
Immunocompetent adults presenting with abdominal pain and fever.
Combination of ceftriaxone and metronidazole followed by escalation to cefoperazone-sulbactam post-splenectomy.
Clinical Best Practices
Consider splenic abscess in patients with recurrent pleural effusion and fever.
Ensure timely surgical intervention in cases of culture-negative abscess.