Clinical Scorecard: Report on a Case of Concurrent Intramucosal Gastric Cancer Linked to Epstein–Barr Virus Identified Following Brief Helicobacter pylori Treatment
At a Glance
Category
Detail
Condition
Epstein–Barr virus-associated gastric cancer (EBVaGC)
Key Mechanisms
Characterized by prominent lymphoid stromal infiltration, extensive CpG island methylation, PIK3CA mutations, and high PD-L1/PD-L2 expression.
Target Population
Predominantly affects males, particularly in the proximal gastric body or remnant stomach.
Care Setting
Endoscopic assessment and treatment of gastric lesions.
Key Highlights
EBVaGC accounts for approximately 8.7% of gastric cancers worldwide.
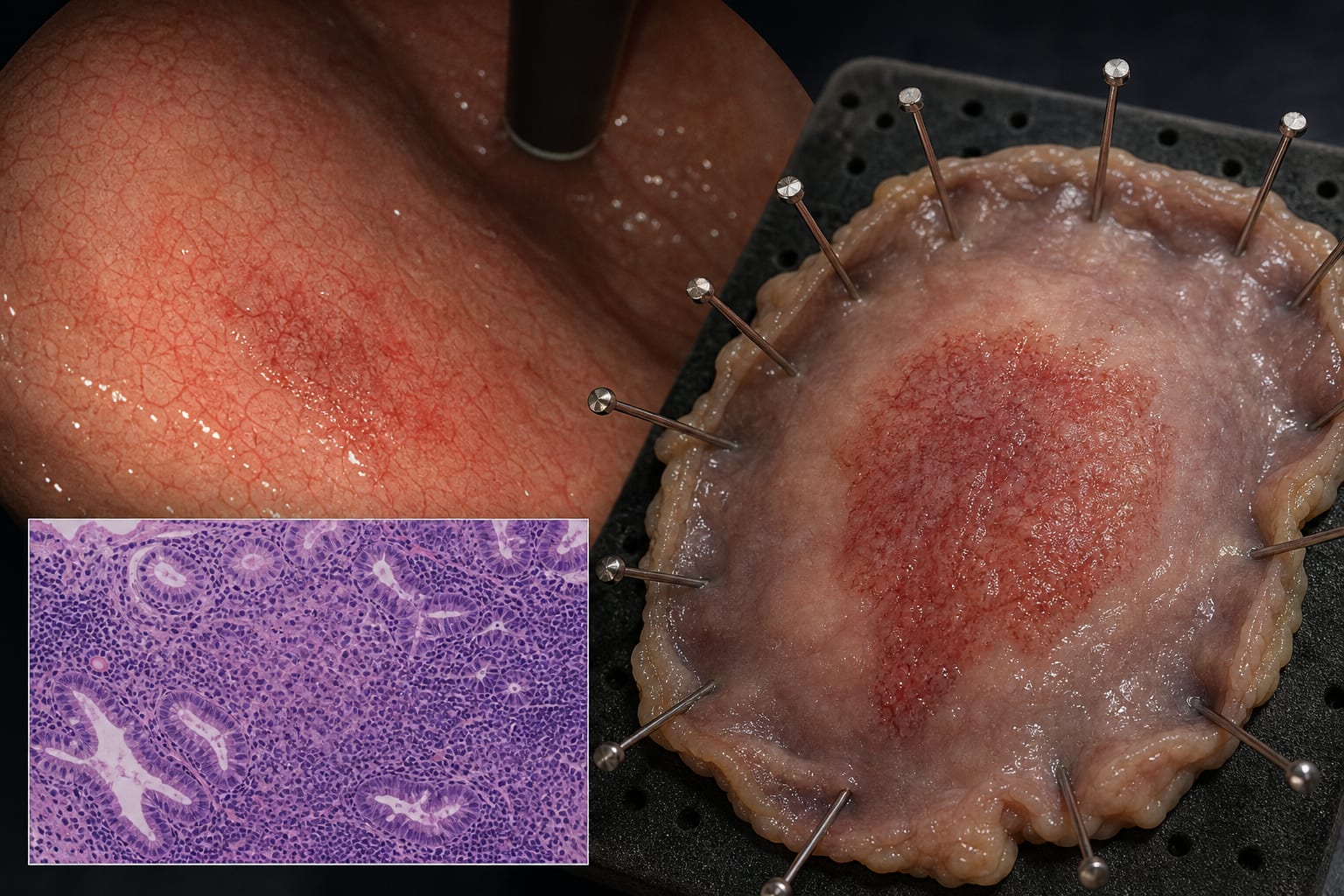
Endoscopically presents as superficial depressed lesions or submucosal tumor-like masses.
Successful curative resection achieved via endoscopic submucosal dissection (ESD) after Helicobacter pylori eradication.
Active HP gastritis can obscure neoplastic lesions, complicating diagnosis.
EBV status serves as a favorable prognostic indicator.
Guideline-Based Recommendations
Diagnosis
Definitive diagnosis relies on strong nuclear EBER expression by in situ hybridization.
Management
Endoscopic submucosal dissection (ESD) is a curative modality for early EBVaGC.
Monitoring & Follow-up
Follow-up for recurrence is essential post-curative resection.
Risks
Active HP gastritis may obscure minute neoplastic lesions and blur demarcation lines.
Patient & Prescribing Data
56-year-old male with a history of gastric adenocarcinoma.
Received a 2-week HP eradication regimen prior to ESD.
Clinical Best Practices
Consider HP eradication prior to ESD to improve lesion detection and margin delineation.
Utilize magnifying endoscopy with narrow-band imaging for better assessment of gastric lesions.