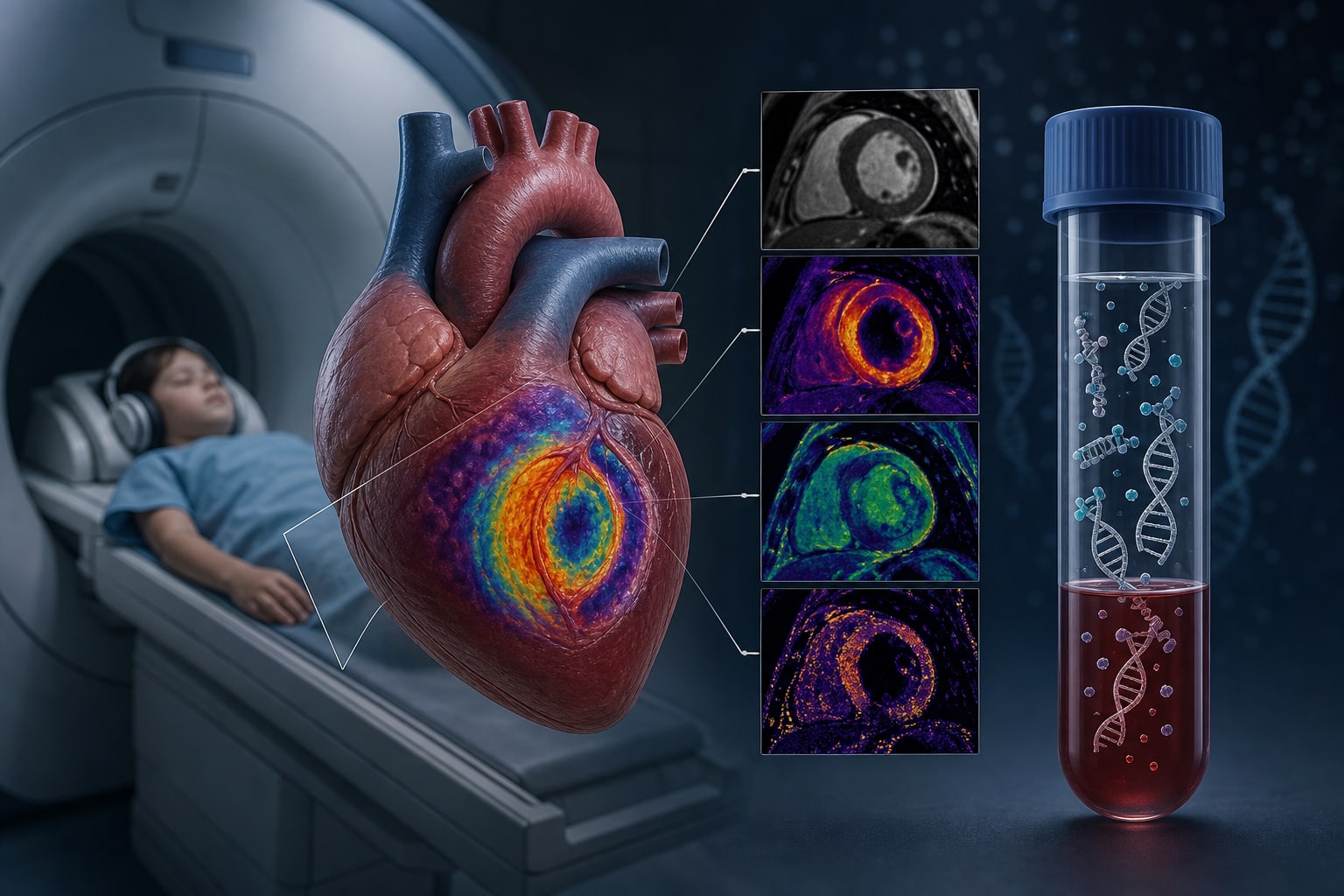
Abnormal Cardiac Magnetic Resonance Imaging Mapping Parameters in Pediatric Heart Transplant Patients with Elevated Donor-Derived Cell Free DNA
By
Kae Watanabe
Defne A. Magnetta
Christina Laternser
Alona Birjiniuk
Joshua D. Robinson
Cynthia K. Rigsby
Nazia Husain
July 9, 2026
Clinical Scorecard: Altered Cardiac MRI Mapping Metrics in Pediatric Heart Transplant Recipients with Increased Levels of Donor-Derived Cell-Free DNA
At a Glance
Category Detail
Condition Pediatric Heart Transplantation Key Mechanisms Utilization of donor-derived cell-free DNA (ddcfDNA) and multiparametric cardiac magnetic resonance imaging (CMR) for rejection surveillance. Target Population Pediatric heart transplant recipients aged 18 years or younger. Care Setting Single center retrospective study evaluating non-invasive surveillance methods.
Key Highlights
High ddcfDNA levels correlate with increased history of cardiac allograft vasculopathy (CAV) and moderate/severe rejection. CMR is performed biennially as an alternative to invasive endomyocardial biopsy (EMB) in select patients. DdcfDNA testing is routinely conducted every 3-4 months to enhance rejection surveillance. Guideline-Based Recommendations
Diagnosis
Rejection defined by ISHLT scoring of ≥ 2R Acute Cellular Rejection (ACR) or any antibody mediated rejection (AMR). Management
Consider CMR as a non-invasive alternative for rejection surveillance in pediatric heart transplant recipients. Monitoring & Follow-up
Routine ddcfDNA testing at every clinic visit to monitor for rejection. Risks
Increased risk of rejection associated with elevated ddcfDNA levels. Patient & Prescribing Data
Pediatric heart transplant patients with varying levels of ddcfDNA.
High ddcfDNA levels indicate a need for closer monitoring and potential intervention.
Clinical Best Practices
Utilize CMR for comprehensive myocardial assessment in pediatric heart transplant recipients. Incorporate ddcfDNA testing into routine surveillance protocols. Related Resources & Content