Clinical Scorecard: Severe Hypertriglyceridemia Linked to Asparaginase in Children with Acute Lymphoblastic Leukemia: Insights from a Single-Center Study
At a Glance
Category
Detail
Condition
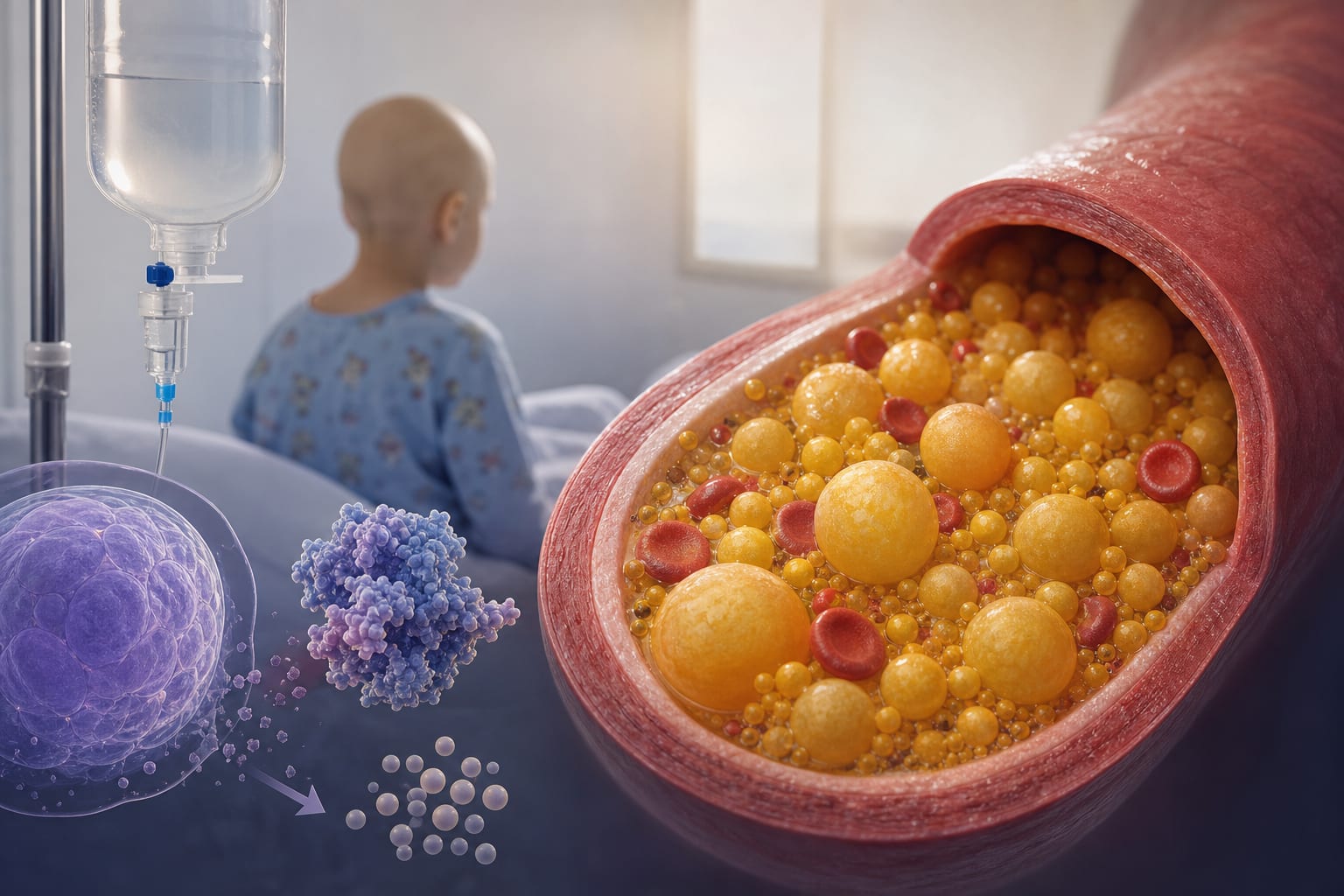
Severe Asparaginase-Induced Hypertriglyceridemia (AIHTG)
Key Mechanisms
Inhibition of lipoprotein lipase function and enhanced hepatic VLDL production.
Target Population
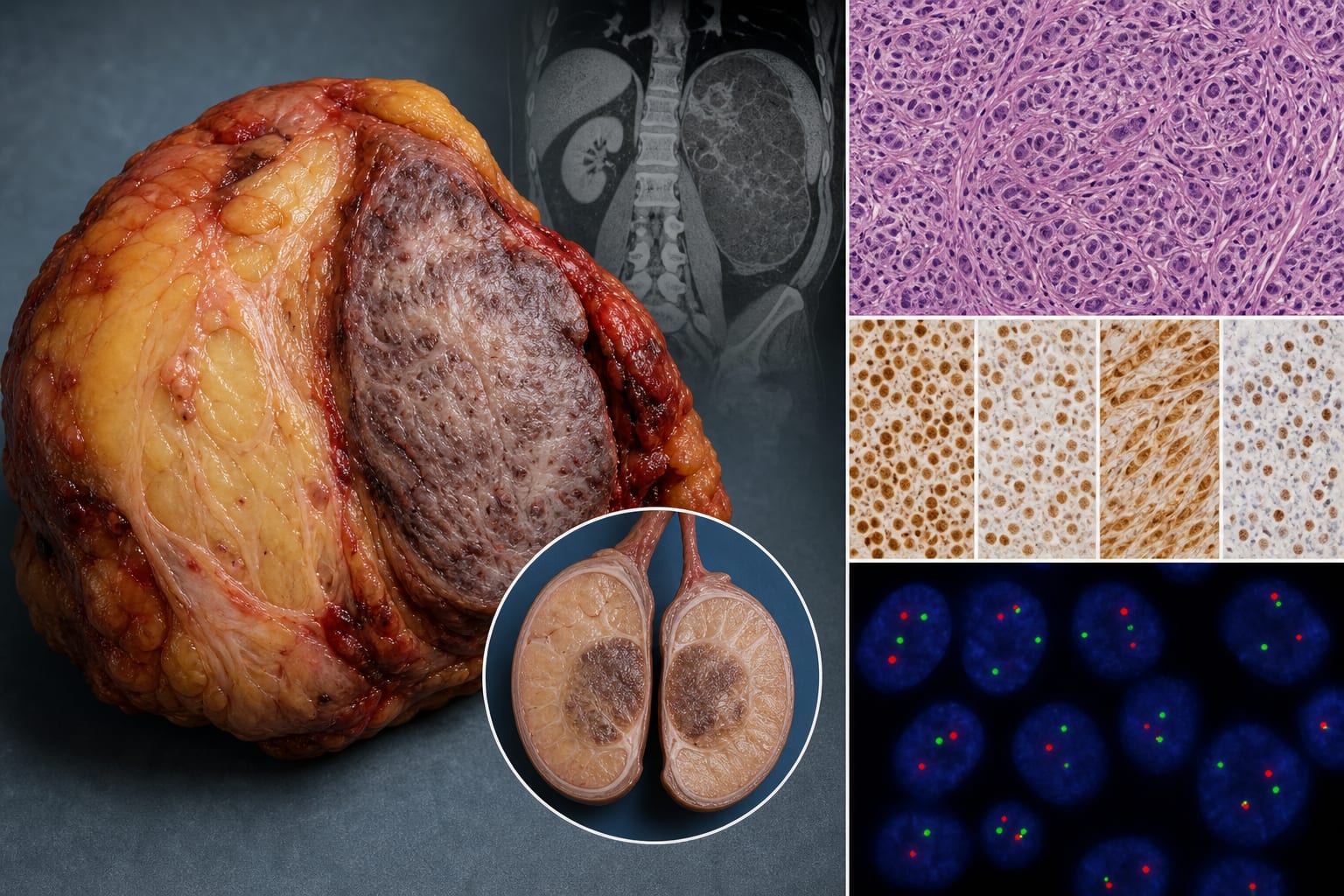
Pediatric patients (≤18 years) with Acute Lymphoblastic Leukemia (ALL).
Care Setting
Oncology treatment center.
Key Highlights
Incidence of severe AAHTG in pediatric ALL patients was 2%.
83% of cases were asymptomatic, detected incidentally.
Median peak triglyceride concentration was 2,645 mg/dL.
Management included intravenous fluids, omega-3 fatty acids, fibrates, and insulin infusion.
Plasmapheresis was performed in three patients with triglycerides >6,000 mg/dL.
Guideline-Based Recommendations
Diagnosis
Severe AAHTG characterized by triglyceride levels exceeding 1,000 mg/dL.
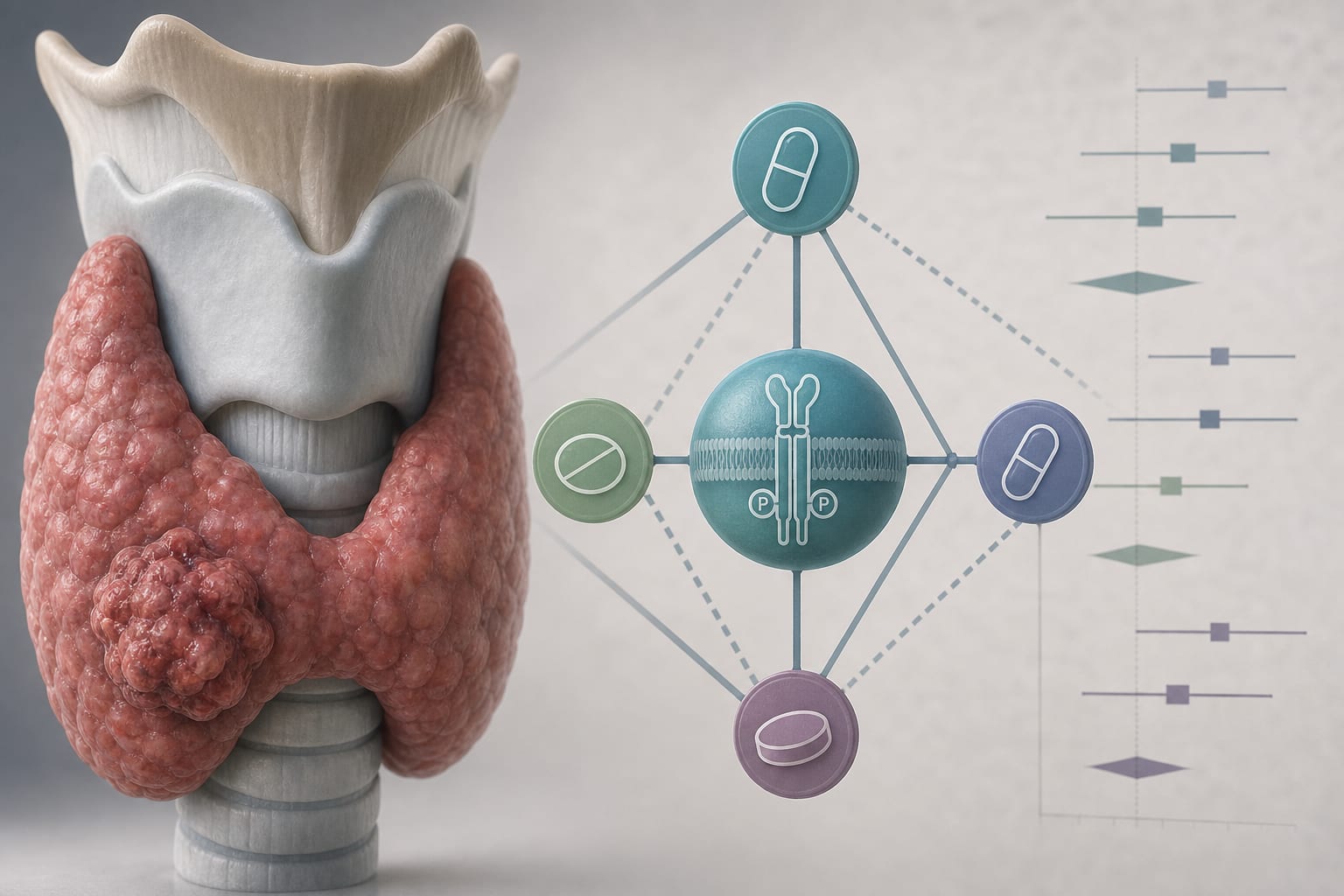
Management
Immediate intervention with intravenous fluids, omega-3 fatty acids, fibrates, and insulin infusion.
Monitoring & Follow-up
Routine triglyceride monitoring is recommended following asparaginase administration.
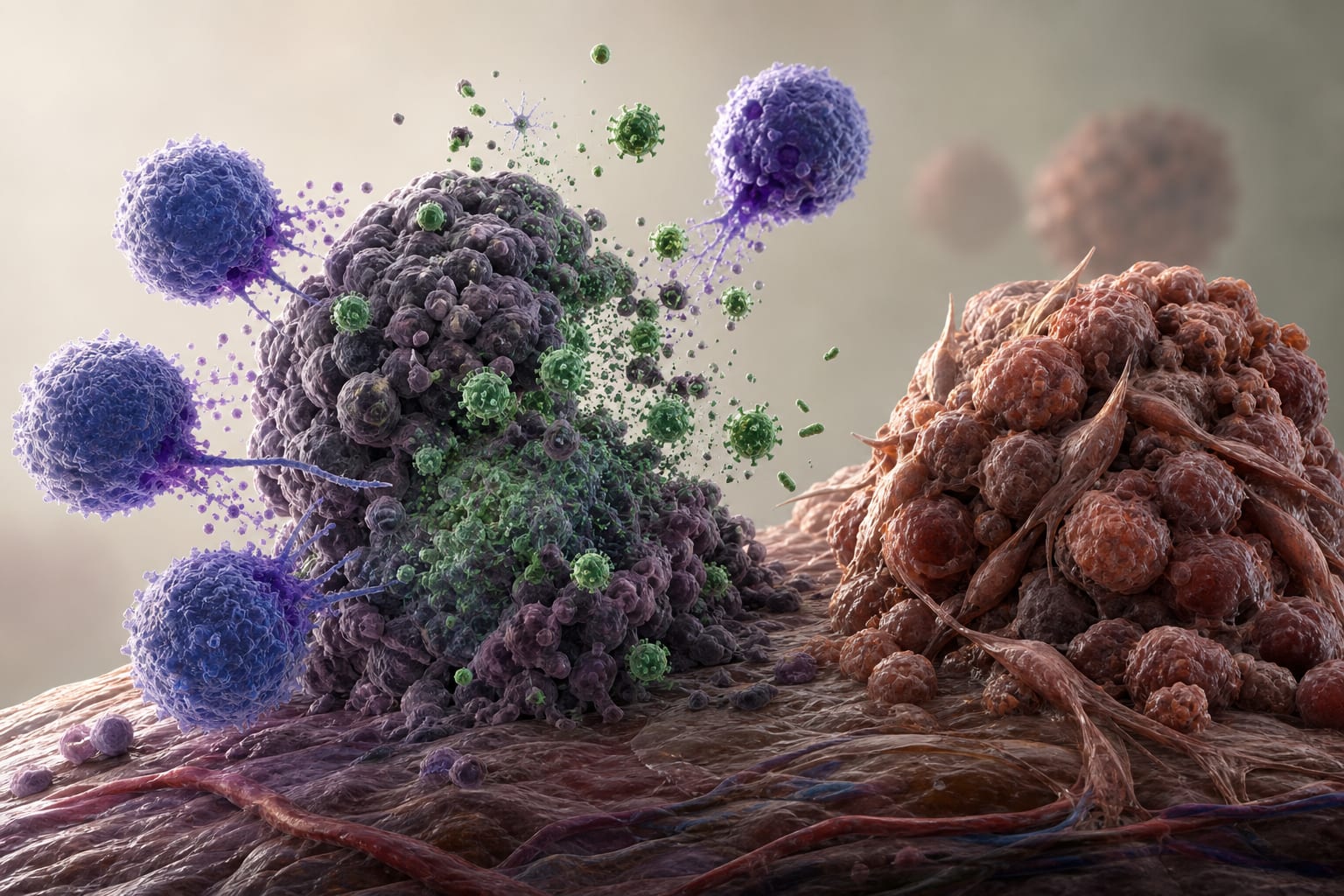
Risks
Potential complications include acute pancreatitis, thrombosis, and hyperviscosity syndrome.
Patient & Prescribing Data
Pediatric patients diagnosed with ALL at King Hussein Cancer Center.
Asparaginase can be reinstated after AAHTG if triglyceride levels are confirmed below 1,000 mg/dL.
Clinical Best Practices
Timely detection of AAHTG through routine lab assessments.
Immediate intervention upon detection of severe hypertriglyceridemia.
Consideration of asparaginase formulation effects on hypertriglyceridemia risk.