Initial observations on dose optimization in 125I seed implantation for recurrent glioblastoma: safety and efficacy across low- and high-dose ranges - Scorecard - MDSpire
Advertisement
Initial observations on dose optimization in 125I seed implantation for recurrent glioblastoma: safety and efficacy across low- and high-dose ranges
Clinical Scorecard: Evaluating Safety and Efficacy of Dose Adjustment in 125I Seed Implantation for Recurrent Glioblastoma: Insights from Low- and High-Dose Applications
At a Glance
Category
Detail
Condition
Recurrent Glioblastoma
Key Mechanisms
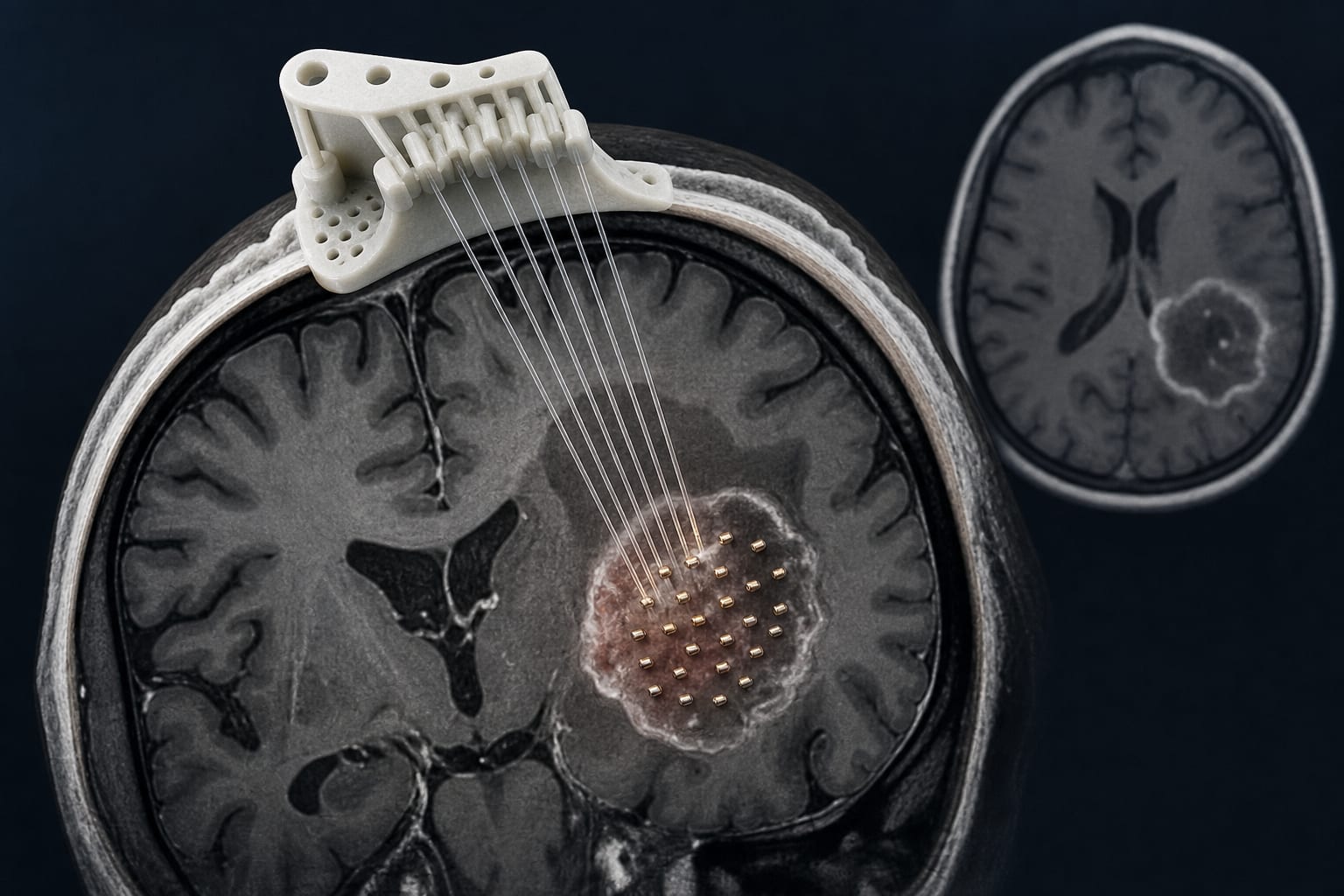
Iodine-125 (125I) seed implantation as a locoregional treatment modality.
Target Population
Patients with recurrent glioblastoma who have received prior treatment.
Care Setting
Retrospective analysis of clinical outcomes in a specialized medical facility.
Key Highlights
The 6-month objective response rate (ORR) was 61.9% for low-dose and 73.2% for high-dose groups.
The 1-year survival rate was 42.9% for low-dose and 68.3% for high-dose groups.
Median overall survival was longer in the high-dose group (13.7 months vs. 11.2 months).
Higher doses increased the risk of postoperative brain edema, manageable with corticosteroids and mannitol.
Guideline-Based Recommendations
Diagnosis
Confirm tumor recurrence using MRI and histological assessment.
Management
Consider 125I seed implantation as a salvage treatment option for recurrent glioblastoma.
Monitoring & Follow-up
Monitor for complications such as symptomatic brain edema post-implantation.
Risks
Increased risk of brain edema with higher dose applications.
Patient & Prescribing Data
62 patients with recurrent glioblastoma treated with 125I seed implantation.
Patients stratified into low-dose (120–140 Gy) and high-dose (140–160 Gy) groups.
Clinical Best Practices
Utilize 3D-printed templates for accurate seed implantation.
Administer corticosteroids and mannitol for managing postoperative brain edema.