Contrast extravasation on CT and angiography as a surrogate marker of bleeding severity
Target Population
Patients with acute bleeding undergoing transarterial embolization
Care Setting
Tertiary referral centers with specialized interventional radiology services
Key Highlights
Endovascular embolization is a highly effective, less invasive treatment for acute bleeding with >95% technical success.
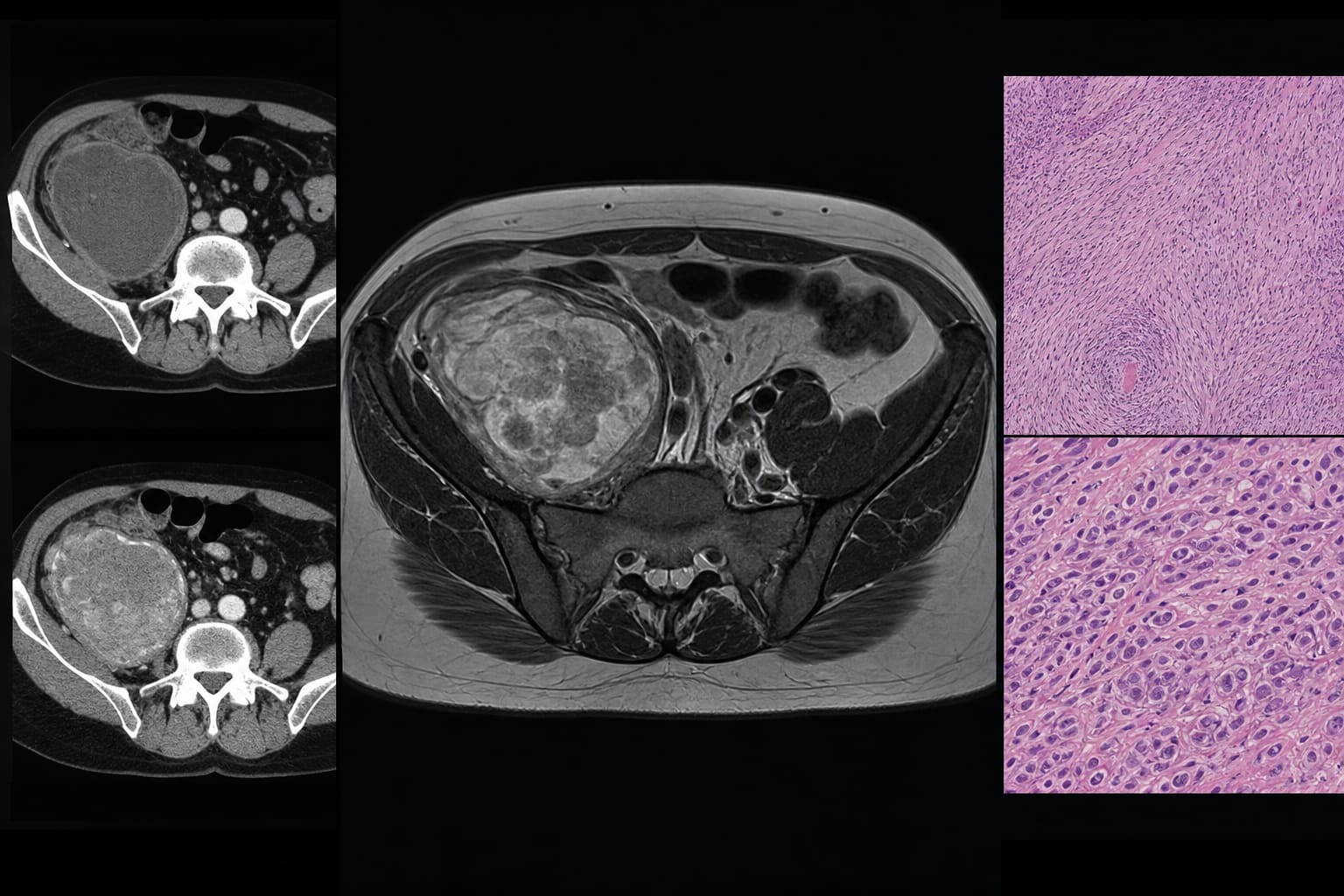
Contrast-enhanced CT has ~95% sensitivity for detecting clinically relevant acute bleeding and is routinely used for localization and procedural planning.
Contrast extravasation volume on CT may serve as a prognostic imaging biomarker correlating with bleeding severity, hemostatic therapy needs, and massive transfusion.
Guideline-Based Recommendations
Diagnosis
Perform multi-slice contrast-enhanced CT within 24 hours prior to angiography to localize bleeding and assess contrast extravasation.
Use triphasic CT imaging (native, arterial, portal-venous phases) for comprehensive evaluation.
Define acute bleeding by clinical symptoms, hemoglobin drop ≥16.1 g/L within 24 hours, hemorrhagic shock signs, or uncontrolled bleeding on endoscopy.
Management
Indicate transarterial embolization (TAE) for acute arterial bleeding refractory to conservative, surgical, or endoscopic treatment or recurrent bleeding.
Select embolic agents based on vascular anatomy, hemodynamics, microcatheter stability, bleeding mechanism, and interventionalist experience.
Perform TAE by experienced interventional radiologists using transfemoral or transbrachial access and appropriate microcatheters.
Monitoring & Follow-up
Monitor clinical signs of shock, hemoglobin levels, coagulation parameters (aPTT, prothrombin time), and transfusion requirements.
Evaluate for massive transfusion needs defined as ≥10 units PRBC in 24 hours or ≥5 units in 4 hours.
Assess 30-day all-cause mortality as a primary endpoint for prognostic evaluation.
Risks
Recognize variable clinical outcomes despite high technical success of embolization.
Consider limitations of CT sensitivity in very low bleeding rates or venous bleeding sites.
Account for patient comorbidities including anticoagulant or antiplatelet medication use.
Patient & Prescribing Data
Patients undergoing TAE for acute hemorrhage with available contrast-enhanced CT imaging within 24 hours.
Contrast extravasation volume on CT may predict bleeding severity and guide hemostatic therapy and transfusion strategies.
Clinical Best Practices
Use multidisciplinary team decision-making incorporating clinical, endoscopic, CT, and angiographic findings for TAE indication.
Ensure CT imaging is performed with contrast and within 24 hours prior to angiography for optimal assessment.
Employ experienced interventional radiologists and tailor embolic materials to individual patient anatomy and bleeding characteristics.
Utilize contrast extravasation volumetry as a potential prognostic tool pending further validation.
by Hans-Jonas Meyer, Simon Riegelbauer, Matthias Mehdorn, Hans-Michael Tautenhahn, Uwe Scheuermann, Silke Zimmermann, Sebastian Ebel, Timm Denecke, Manuel Florian Struck