Clinical Scorecard: Combination of Icaritin and TACE Enhances Survival in Advanced HCC with Macrovascular Invasion: Findings from a Multicenter Cohort Analysis
At a Glance
Category
Detail
Condition
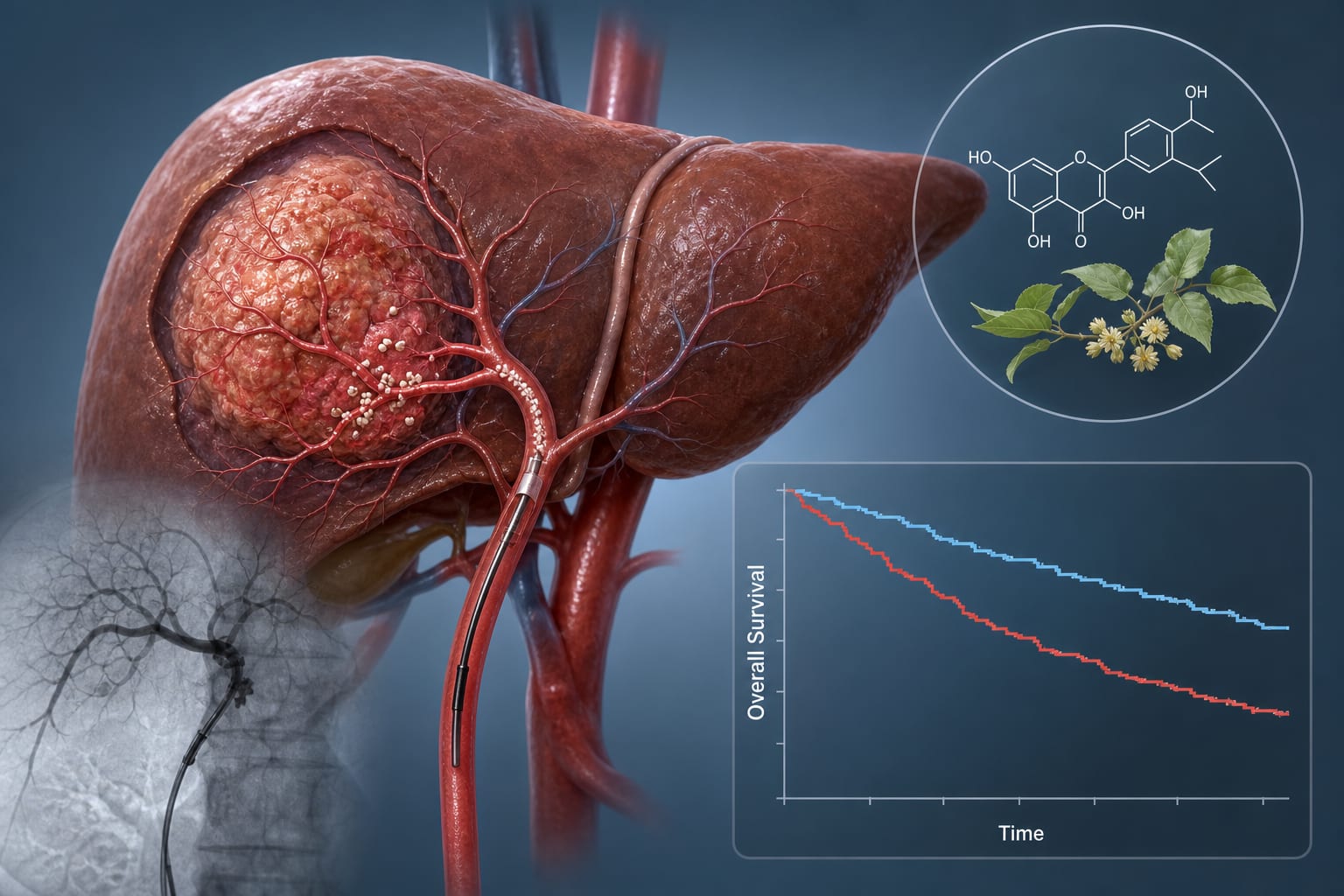
Hepatocellular carcinoma (HCC) with macrovascular invasion (MVI)
Key Mechanisms
Icaritin induces apoptosis and modulates immunity, enhancing antitumor activity.
Target Population
Patients with HCC and MVI, aged 18 to 80 years, with ECOG performance score of 0-1 and Child-Pugh class A or B.
Care Setting
Multicenter tertiary hospitals
Key Highlights
Icaritin combined with TACE significantly improves overall survival (OS) and progression-free survival (PFS).
Median OS was 16.3 months for Icaritin-TACE group vs. 13.3 months for TACE alone.
Disease control rate (DCR) was higher in the Icaritin-TACE group (84.0% vs. 72.2%).
Independent predictors of OS include ECOG performance status, AFP levels, number of lesions, and maximum lesion diameter.
Overall incidence of adverse events was similar between both treatment groups.
Guideline-Based Recommendations
Diagnosis
Diagnosis of HCC confirmed by histology or imaging with MVI.
Management
Icaritin is recommended in the treatment of advanced HCC according to the 2022 Guidelines for the Diagnosis and Treatment of Primary Liver Cancer.
Monitoring & Follow-up
Monitor serum AFP levels and assess performance status.
Risks
Exclusion criteria include extensive portal vein tumor thrombus, coagulation dysfunction, and active infections.
Patient & Prescribing Data
288 patients with HCC and MVI from five tertiary hospitals.
Icaritin was prescribed based on local institutional practice and physician assessment.
Clinical Best Practices
Assess liver function and performance status before prescribing Icaritin.
Consider combination therapy with TACE for patients with MVI to improve survival outcomes.